INTRODUCTION
Dural arteriovenous fistulas (AVFs) are abnormal direct continuations of arteries and veins within the dura. Dural AVFs account for approximately 10% to 15% of all intracranial arterio venous malformations8,13). The common treatment modalities for dural AVFs include surgical resection, endovascular embolization, radiation therapy, and conservative clinical management.
Multiple dural AVFs are very rare and hard to treat; these cases account for 6% to 9% of all cases of dural AVFs1,5,15). Patients with multiple dural AVFs have a high risk of hemorrhage, which includes venous obstruction1), and aggressive treatment modalities are often required to improve neurological and cognitive symptoms in these patients4).
The common initial symptoms of AVFs are headaches, tinnitus, proptosis, and intracranial hemorrhage3,8,14). Several cases of dural AVFs accompanied by cognitive symptoms such as dementia, Parkinsonism, amnesia, and alexia have been reported6,7,9-12,16,17). However, to our knowledge, there have been no reports on schizophrenia as a presenting symptom of dural AVFs so far.
In this study, we report our experience with a patient presenting with multiple dural AVFs and schizophrenia-like symptoms, who was treated using a staged and active treatment strategy.
CASE REPORT
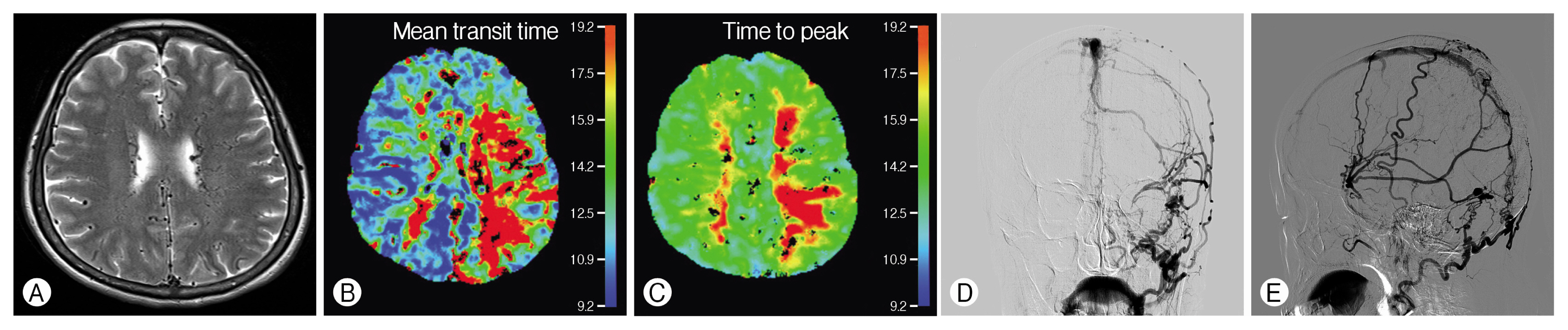
A 51-year-old woman presented with visual disturbances that had persisted for approximately one year. She was under treatment with the following psychiatric medications: paliperi-done (9mg, QD), benztropine mesylate (2mg, QD), lorazepam (1mg, QD), quetiapine fumarate (100mg, QD), trazodone hydrochloride (25mg, QD), and propranolol hydrochloride (20mg, BID); these drugs were being administered for the treatment of schizophrenia at a psychiatric hospital. The patient had been showing symptoms of delusion, negative symptoms, and dysphoric mania for an 11-year period. Brain magnetic resonance imaging (MRI) was performed at a previous hospital because the patient experienced visual disturbances. The initial MRI scans showed vasogenic cerebral edema in the left temporo-occipital area and engorged vessels in both cerebral hemispheres. The patient was then transferred to our research hospital for additional examinations. Subsequent MRI scans of the brain confirmed the presence of engorged vessels in both cerebral hemispheres and a delay in the mean transit time (MTT) and time to peak (TTP) on perfusion images (Fig. 1A-C). We also performed transfemoral cerebral angiography (TFCA) examinations as we suspected the presence of dural AVFs. The TFCA revealed multiple dural AVFs, along with cortical reflux and venous ectasia. The feeding arteries identified were as follows: both middle meningeal arteries (MMAs), superficial temporal arteries (STAs), and occipital arteries (OAs). The superior sagittal sinus (SSS) was the draining vein. In the right internal carotid artery (ICA), early enhancement of the SSS and cortical vein drainage were observed, but no feeding artery was present. In the right external carotid artery (ECA), the fistula penetrated through the bone to the SSS from the right STA parietal branch. In the SSS, the fistula penetrated from the right MMA posterior branch, and through the bone from the right OA. In the left ICA, there was an early enhancement of the SSS and cortical vein drainage, but no feeding artery was observed. In the left ECA, the fistula penetrated through the bone to the SSS from the left STA parietal branch and the fistula in the SSS from the left anterior and posterior MMA branches. The fistula penetrating through the bone from the left OA and venous ectasia were located around the transverse sigmoid sinus junction, and early enhancement of the SSS and cortical vein drainage were observed (Fig. 1D, F).
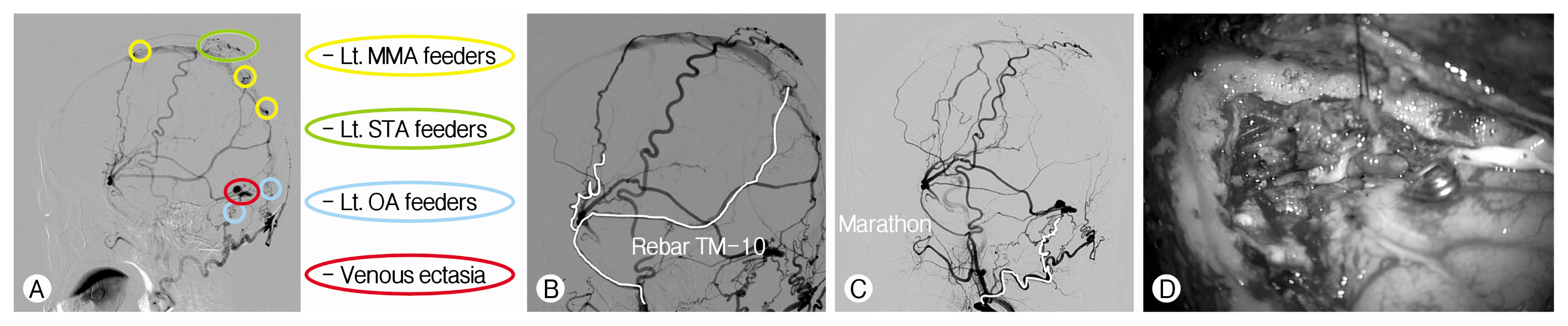
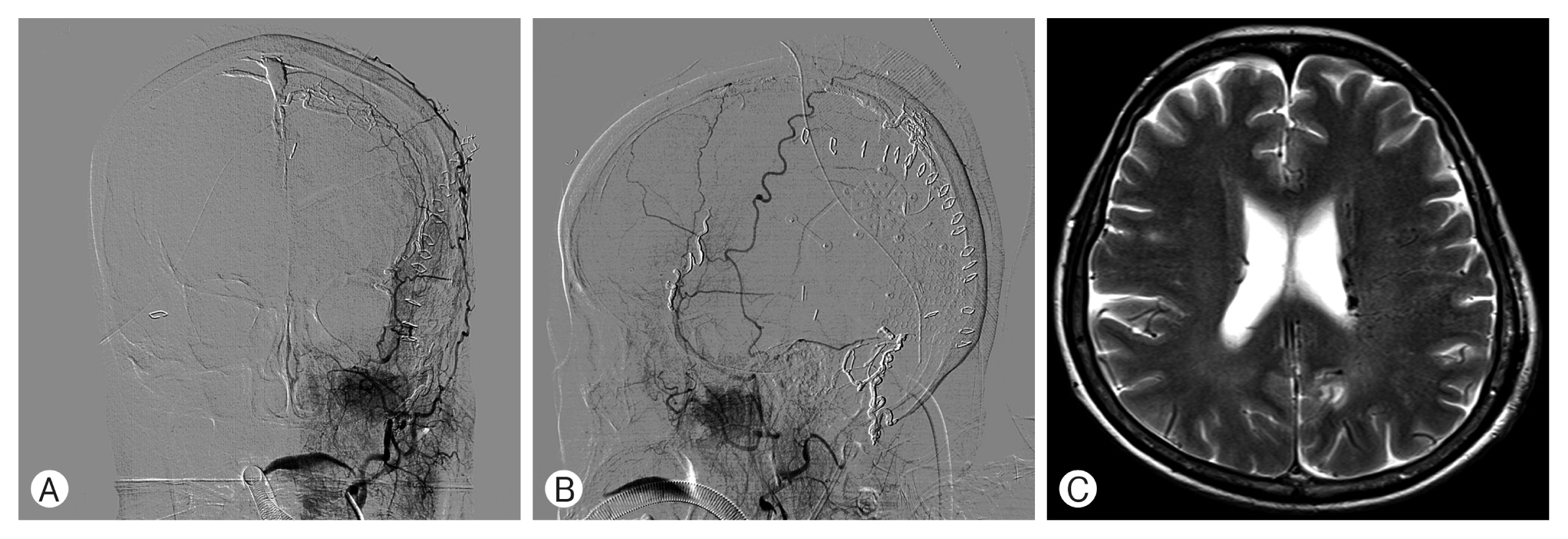
It appeared that the feeder arteries of the left ECA were the main feeder arteries of the AVFs, and we therefore planned a stepwise treatment. The feeder arteries included the left MMA, the left STA, the left OA, and the venous ectasia (Fig. 2A). In order to accomplish this, we first performed Onyx embolization of the left MMA. We then used the steerable vascular Rebar microcatheter for the left MMA anterior and posterior branches (Fig. 2B). Subsequently, we performed an ultrasound-guided surgical ligation of the left STA using the Doppler system under local anesthesia. Finally, we performed Onyx embolization of the left OA using a Marathon microcatheter platform (Fig, 2C), and we then clipped the venous ectasia using navigation system, under general anesthesia (Fig. 2D). Postoperative TFCA showed no fistula on the left STA, MMA, OA, or venous ectasia, and instead showed a marked decrease in cortical draining veins (Fig. 3A, B). Follow-up brain MRI performed 20 days after the surgery showed a prominent decrease in engorged vessels in both hemispheres, compared to the initial MRI scan (Fig. 3C).
After the surgery, the patient’s schizophrenia symptoms were improved. Remarkably, although the patient stopped taking the schizophrenia medication that was initially prescribed, she could express her thoughts logically, could express her emotions precisely, and her delusions also disappeared.
DISCUSSION
As mentioned above, dural AVFs are associated with symptoms such as headaches, tinnitus, proptosis, and intracranial hemorrhage along with a decrease in cognitive functions3,6-12,14,16,17).
The patient evaluated in this study was thought to have schizophrenia and was under treatment with psychiatric medication for 11 years. Although we searched the medical and scientific literature for any cases of dural AVFs accompanied by schizophrenia symptoms, no such case was found.
Initial TFCA revealed that the patient in this case had multiple dural AVFs, which are extremely rare and have a high probability of a malignant outcome. Therefore, aggressive treatment modalities are recommended for the clinical management of multiple dural AVFs4).
Typically, the classification of dural AVF is determined by the venous drainage pattern, which determines the severity of the condition. There are two classification schemes, based on the Borden and Cognard system. In the present case, the dural AVF was drained from the MMA to the cortical vein with venous ectasia, which is classified as Borden type 3 and Cognard type 42,3).
In this case, the feeder arteries of the left ECA were thought to be the main feeder arteries; consequently, we planned a staged and aggressive treatment. During the intervention, starting with the first Onyx embolization, the previously prescribed anti-schizophrenia medication was stopped and the patient’s schizophrenia symptoms worsened; these were brought under control only after the patient restarted the psychiatric medication.
However, after completion of the Onyx embolization along with the surgical ligation and clipping of the venous ectasia, the patient’s symptoms of schizophrenia were markedly improved. Although she had stopped taking the psychiatric medication, she could express herself logically, could express her emotions precisely, and her delusions also disappeared.
It is possible that the patient could have been misdiagnosed with schizophrenia, although she showed decreased cognitive function when she first arrived at our hospital. Another possibility is that the improved cerebral blood flow after treatment had a significant effect on her schizophrenia symptoms.
CONCLUSION
Here, we reported a case of multiple dural AVFs presenting with schizophrenia symptoms. In this case, we used a staged and aggressive treatment that was effective in treating the condition and achieved significant improvement of associated symptoms. Brain MRI can be helpful in making an accurate diagnosis in cases where decreased cognitive functions or mental illness are present. We suggest that multiple dural AVFs should be actively treated in order to improve the symptoms.