INTRODUCTION
Intraocular melanomas are the most common primary ocular malignancy in adults, but accounts for 5% of all malignant melanomas6). Approximately 95% of melanoma around the eye is found in the uvea, and choroid melanoma is the most common primary ocular malignancy in adults. In many cases, the predominant site of metastatic disease for patients with choroid melanoma is the liver. Spinal/vertebral metastasis is an infrequent clinical entity. Spinal metastasis of choroid malignant melanoma has been reported only in 3 previous cases2,3). However, previous reports have discussed thoracic spine metastasis. To our knowledge, this is the first report of the lumbar spine as the main lesion location without thoracic or cervical spine symptoms.
CASE REPORT
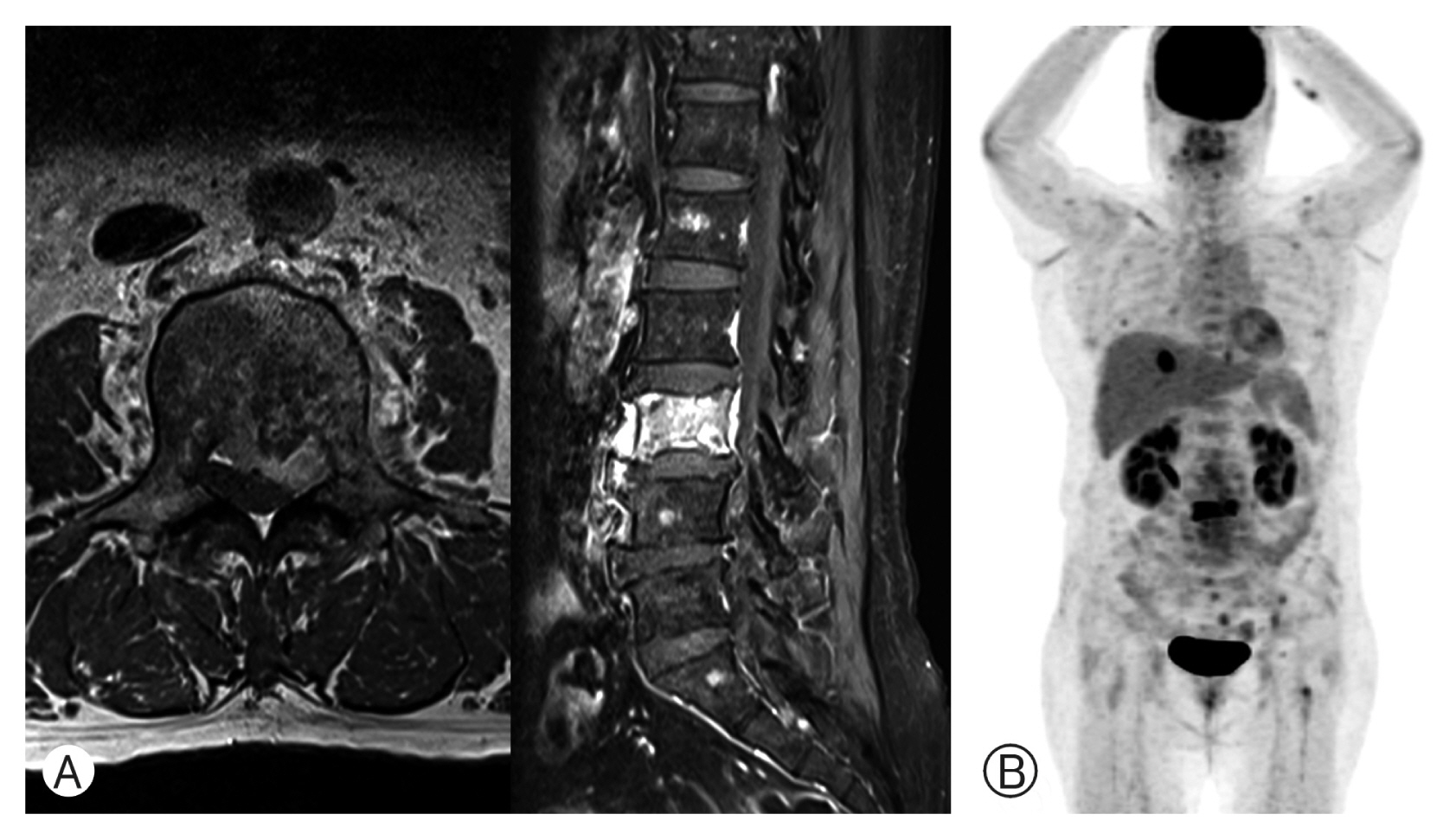
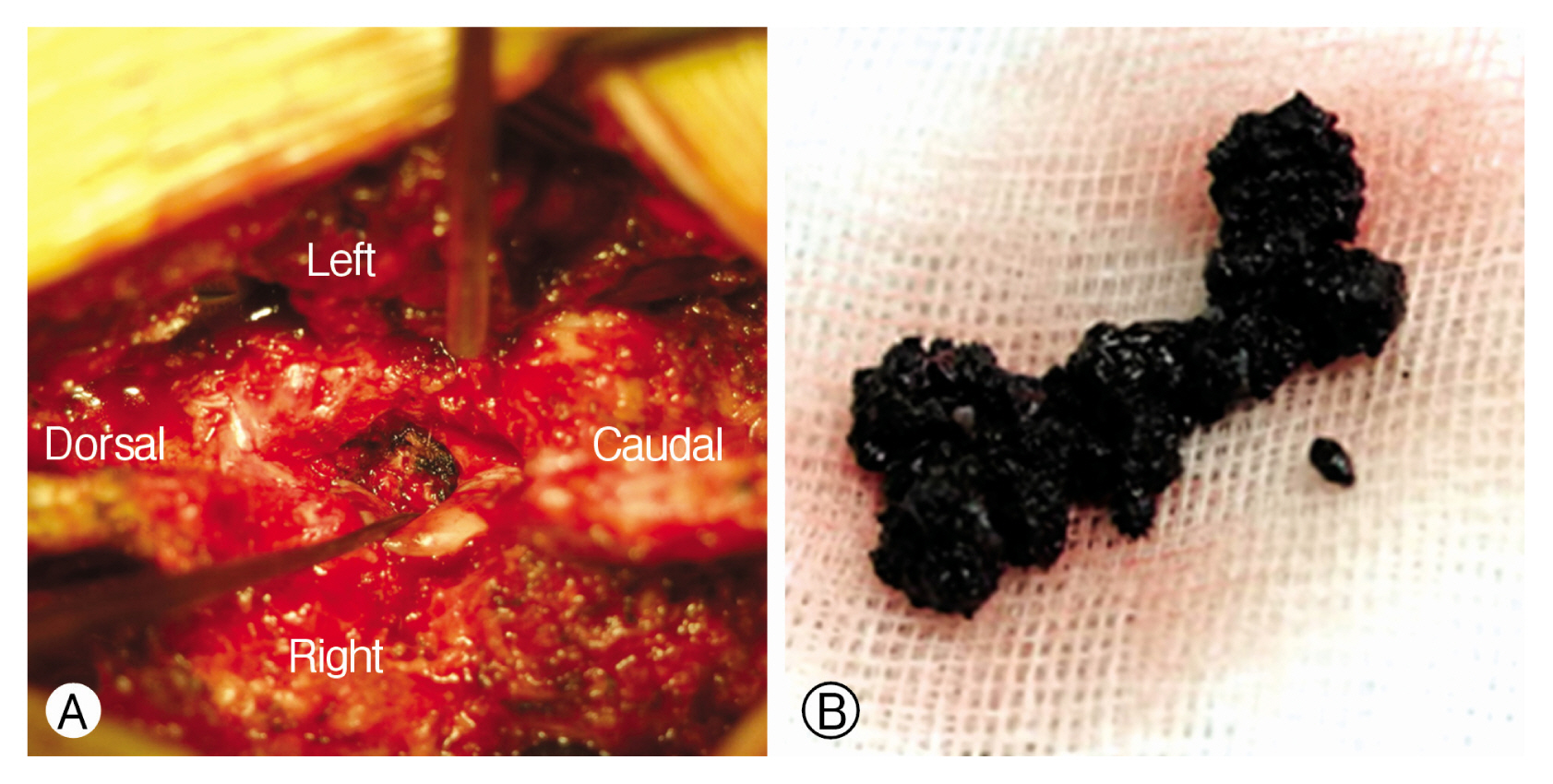
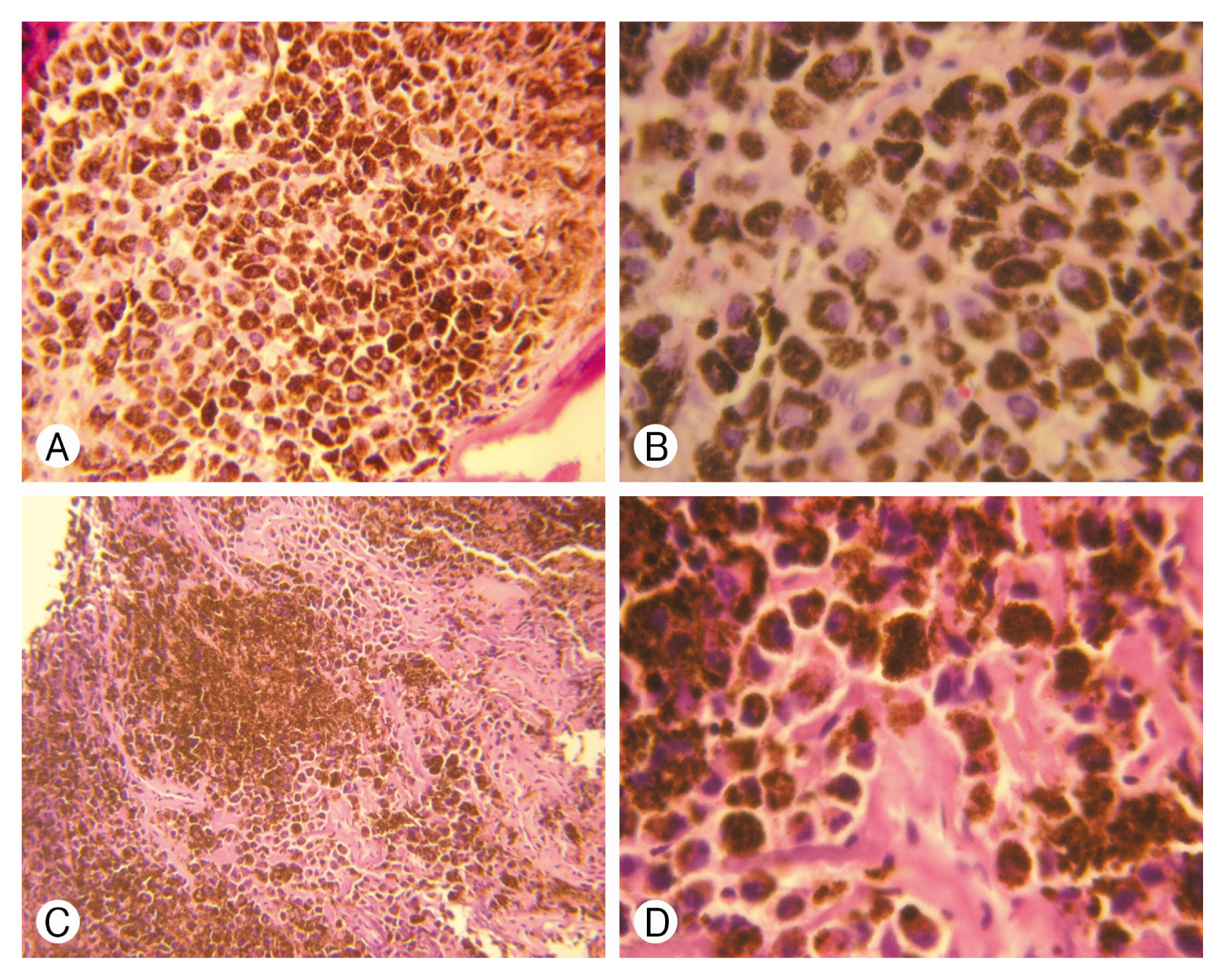
A 57-year-old woman visited our hospital with left flank pain and left anterior thigh and calf radiation pain that had persisted for one month. There was no history of trauma or fall. She was admitted to the hospital and underwent lumbar spine magnetic resonance imaging (MRI). The T1-weighted image (WI) showed a body fracture line and high-intensity signal at the L3 vertebral body. A low-intensity signal was detected in this area on T2-WI, and contrast MRI showed a heterogeneous enhancing ventral epidural mass compressing the dura posteriorly at the L3 level and totally enhanced the L3 vertebral body (Fig. 1A). Positron emission tomography-computed tomography (PET-CT) showed a contrast of the liver, both ribs, clavicle, sternum, thorax-lumbar-sacrum spine, both pelvic bones, right humeral shaft, and left proximal femur (Fig. 1B). To reduce the patient’s pain, L3 laminectomy, left facetectomy, and partial tumor removal with posterior pedicle screw fixation were performed. After L3 laminectomy, the soft and black-colored mass was presented on vertebral body (Fig. 2A). Immunohistochemistry from the vertebral body showed strongly positive human melanoma black 45 (Fig. 3). And additional histopathological assessment confirmed that it was malignant melanoma (Fig. 2B).
The patient had a history of enucleation of the right eyeball that was diagnosed 8 years prior, the pathology of which identified it as choroid malignant melanoma. Family history revealed that her mother died of pancreatic cancer 40 years previous, and her brother died of liver cancer 2 years prior. Several imaging of the choroid malignant melanoma and PET-CT were performed in the hospital where she had received the first diagnosis, and she received treatment and follow-up for 5 years. After 5 years, the patient achieved complete remission and refused additional follow-up. Thus metastasis could not detected early.
After the operation, her left leg and flank pain was improved, and she was discharged after 10 days without complication. After surgery, radiotherapy (RTx) and chemotherapy (CTx) are being performed at other hospitals, and they have survived more than 1 year after surgery.
DISCUSSION
Choroid melanomas are the most common primary intraocular malignant tumor in adults. While choroid melanomas represent only 5% of all melanomas, they have a high rate of metastasis and poor response to treatment and account for about 13% of melanoma deaths3). Because there is currently a limited amount of data on spinal metastasis from choroid melanomas, treatment for this is similar to that for all types of melanoma to spinal/vertebral metastasis3).
Several studies have suggested that all therapies for uveal melanoma metastasis do not significantly impact overall survival and clinical improvement1,5). In addition, there are a limited number of studies that address the role of surgery for spinal melanoma metastasis6). There is no clear treatment for this reason, but there are studies as follows. One study reported that the number of melanoma metastatic sites is an important prognostic factor, and total tumor removal should be considered in healthy patients with spinal metastasis and surgically resectable tumors limited to one organ8). Another study established that if the entire tumor cannot be removed, direct decompressive surgery plus postoperative RTx for all types of spinal metastasis is superior to radiotherapy alone4). And surgical resection appears to preserve neurological function and can improve overall outcomes from melanoma metastatic to the spine6).
Spinal metastasis of choroid malignant melanoma has been reported in 3 cases, and specific treatment were presented in 2 cases. In 2 cases, tumor removal was performed, but the prognosis was poor (Table 1). One patient died several weeks after surgery, thus RTx and CTx were not performed. And another patient was performed RTx and CTx, but developed multiple metastasis after 7 months.
In our case, due to lack of follow-up, metastasis was not detected early and the patient had already multiple metastasis. Based on the results of previous studies, the tumors were not totally removed and decompressive tumor removal was performed. As in the previous 2 cases, L3 laminectomy, left facetectomy, and partial tumor removal with posterior pedicle screw fixation were performed. After surgery, RTx and CTx are being performed at other hospitals, and they have survived more than 1 year after surgery.
Metastasis caused by choroidal melanoma usually occurs within 5 years after diagnosis, but late metastasis is also a well-known complication. Shields et al. reported a case of orbital recurrence and liver metastasis 42 years after primary tumor enucleation7). In ocular melanoma, the liver is the most common site of metastasis, and only one case of spine metastasis without liver metastasis has been reported3).
In this case, if the metastasis had been identified earlier, it could have been limited to the liver and treated before metastasis to the spine.
CONCLUSION
We report a rare case of spinal metastasis of malignant choroid melanoma. To our knowledge, this is the first report of the lumbar spine as the main lesion location without thoracic or cervical spine symptoms. Unfortunately, due to a lack of follow-up, the metastasis was not detected and treated early. Because melanoma is associated with recurrence, we suggest that future cases of melanoma, even cases that achieve remission, complete follow-up over the patient’s lifetime to detect and treat any recurrence.