INTRODUCTION
Grisel’s syndrome is non-traumatic atlantoaxial subluxation which is predominantly occurred in pediatric patients younger than 12 years old (68%), with 90% of cases under 21 years old. There is no gender predilection for the syndrome16). It is relatively common in children, with an estimated prevalence of 5.6% in the general ophthalmological patients2). Pathogenesis is commonly related to upper respiratory tract infections such as rhinopharyngitis, cervical osteomyelitis, otitis media, or surgical procedures like adenoidectomy, tonsillectomy, repair of choanal atresia, and mastoidectomy. The 48% is secondary to infection and 40% is secondary to surgery (adenotonsillectomy in 78%)2). The main symptom is neck pain, torticollis, limited and painful neck movement and rarely dysphasia. Physical examination shows a spasm of the sternocleidomastoid muscle contralateral to the rotation. The diagnosis is established based on laboratory test to detect signs of infection and radiological approach for visualizing the subluxation. Previously, surgical treatment was considered if the displacement lasted more than three weeks because of the high risk of recurrence and permanent deformity11). We report the 2 cases of Grisel’s syndrome. The first case is a 10-year-old male patient with chronic Grisel’s syndrome for more than 6 months, Fielding type III with atlantodental interval (ADI) over 5 mm treated with conservative treatment without surgical option. The second case is a 5-year-old female patient with acute form of Grisel’s syndrome successfully treated with pain control and halo traction.
CASE REPORT
Case 1
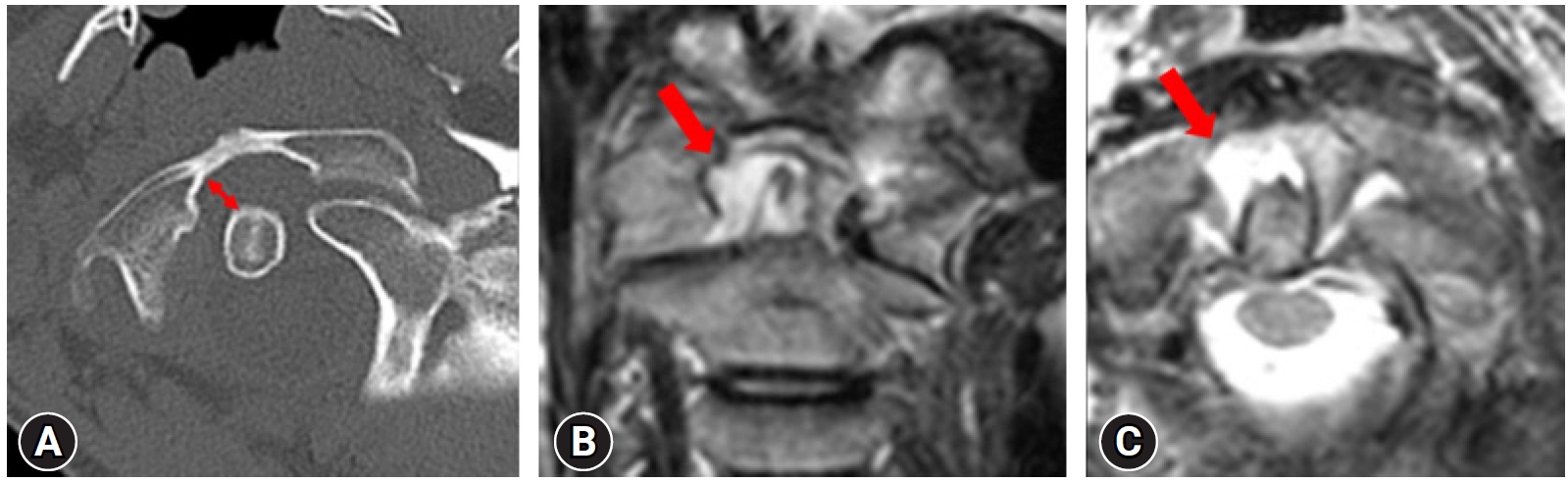
A 10-year-old male patient visited our hospital having complained of torticollis, neck pain, and dysphasia after mastoidectomy due to the removal of cholesteatoma in his left ear 6 month ago. His head was rotated to the left and tilted to the right. He complained of neck pain on attempted motion of the head, dyspnea, dysphagia, snoring and nausea. Because of these symptoms, he lost about 4 kg in two months. He had no history of trauma. Physical examination identified no tonsillar hypertrophy and hyperemia. There was a spasm of the ipsilateral sternocleidomastoid muscle exacerbated by the attempt to perform contralateral active rotation. Laboratory examinations showed absence of leukocytosis (7400/mm3; normal range, 4,000-11,000) and normal C-reactive protein (< 0.03 mg/dL). Computed tomography (CT) obtained demonstrated rotary displacement of the atlas with anterior displacement (fielding type Ⅲ). The ADI was widened over 7 mm and neck was tilted to the right. Magnetic resonance imaging (MRI) showed an inflammatory process in the atlantodental space which extends to involve prevertebral soft tissues (Fig. 1). The patient was placed in soft neck collar and received a conservative treatment consisted of pain control as ibuprofen, a muscle relaxant. Intermittent cervical traction was performed, starting from 0.5 kg/body weight to max 1.5 kg/body weight every day for 2 months. For the next two months, he continued to get traction therapy and take analgesia (ibuprofen). Head rotation and dislocation got corrected and symptoms were dramatically relieved (Fig. 2).
Case 2
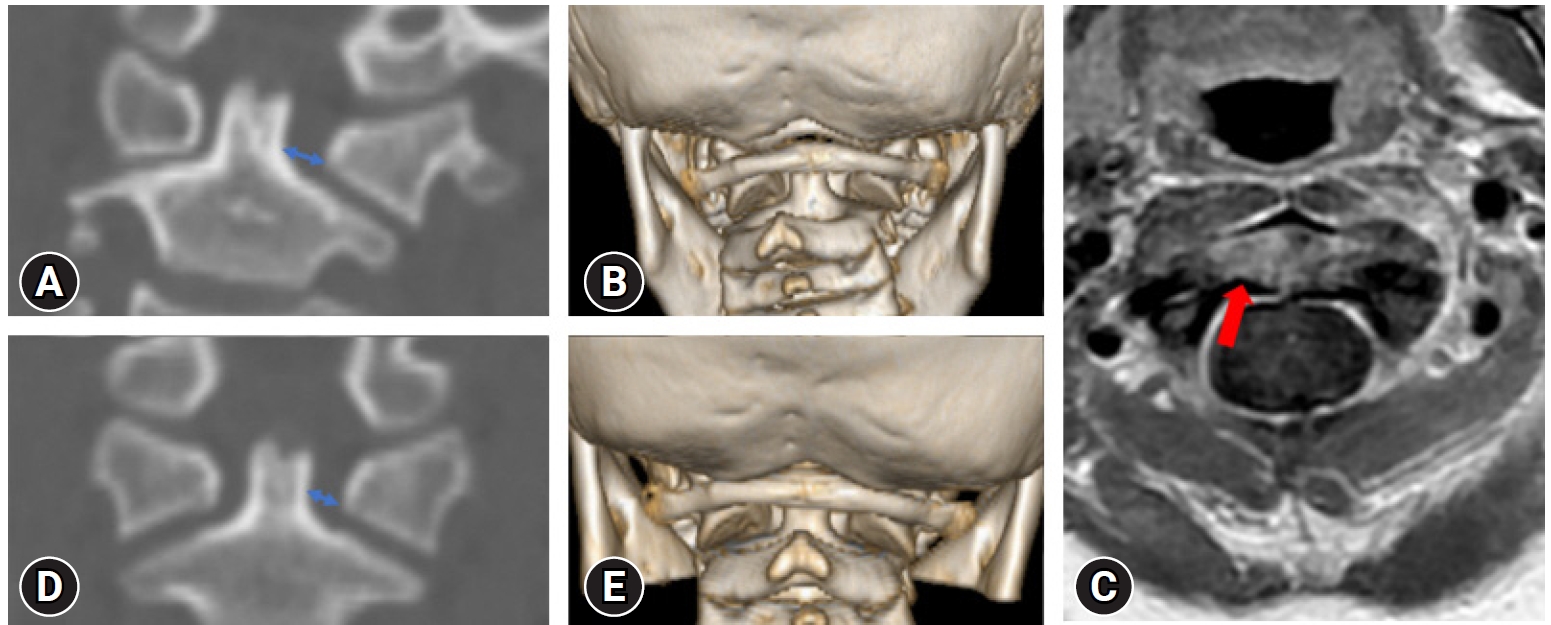
A 5-year-old female child was referred for evaluation of torticollis. She was diagnosed with acute pharyngitis 3 days ago with 39℃ fever and throat pain. Multiple enlarged lymph nodes and pharyngeal hypertrophy were detected. She was treated with intravenous antibiotics (ampicillin and β-lactamase inhibitor) and ibuprofen. Otherwise, the parents said no history of trauma or pre-existing health condition. Physical examination showed limited cervical range of motion. Her head was rotated to the right and tilted to the left. She was neurologically intact and had limited painful neck movement. There was a spasm of sternocleidomastoid muscle when attempt to rotate her neck. Laboratory examination showed leukocytosis 19700/mm3 (normal range, 4,000-11,000) and C-reactive protein 9.67 mg/dL (normal range, < 0.5 mg/dL). CT revealed a rotated head with normal ADI and MRI showed inflammatory change in the bilateral retropharyngeal space with resolved fluid collection (Fig. 3). Conservative care of neck collar and taking ibuprofen was done for 3 weeks but there was no symptomatic improvement and traction therapy was initiated. After intermittent cervical traction with 2 kg and bedside halter traction for 1 week, dislocation was normalized and neck pain and motion limitation were relieved (Fig. 3).
DISCUSSION
Grisel’s syndrome is atlantoaxial rotatory subluxation after infection of the upper respiratory tract. Grisel’s syndrome is generally related to head and neck infections such as pharyngitis, adenotonsillitis, tonsillar abscess, cervical abscess, and otitis media. It has been occurred after numerous otolaryngological procedures such as tonsillectomy, adenoidectomy and mastoidectomy4). There are many mechanisms for Grisel’s syndrome, including expansion of infection to the joints via anastomotic lymphatic and venous channels, synovial inflammation, effusion, distension, and instability of C1-2 joints, post-inflammatory decalcification of the ligamentous insertions inducing articular loosening, and reactive paravertebral muscle spasm strong enough to set off the destabilized joints10). Parke WW et al.12) demonstrated a previously unknown plexus of lympho-venous anastomoses via the pharyngobasilar fascia and the atlanto-occipital membrane that helps hematogenous conduction of local infections of the ear or the pharynx. The cases in this paper were caused by inflammation after the removal of cholesteatoma in his left and after acute pharyngitis.
Pang and Li10) classified the atlantoaxial subluxation into 3 different groups according to the pretreatment time (acute < 1 month, subacute = 1-3 month, chronic > 3 month). Fielding classified atlantoaxial subluxation into four different types. In type I, the atlas is rotated on the odontoid without anterior displacement. In type II, the atlas is rotated on one articular process with 3 to 5 mm anterior dislocation. Type III consists of a rotation of the atlas with anterior displacement greater than 5 mm. Type IV is explained by rotatory fixation with posterior displacement5). Type 1 and 2 of subluxation are most common and neurological symptoms are not available. The spinal cord compression and severe neurological findings can be seen in types 3 and 43). Our first patient had an ADI of 7.2, greater than 5 mm, so it corresponds to type III atlanto-axial subluxation and neurological symptoms like dysphasia, aspiration has been detected. The second patient had no anterior displacement with normal ADI, so it was type I atlantoaxial subluxation.
The treatment of Grisel’s syndrome consists of non-surgeries, including halter traction, cervical brace and skull traction and surgeries (C1-2 arthrodesis). Patients, who present within 1 month from the onset of symptoms, are routinely treated by non-surgeries like analgesics, cervical collar for comfort18). However chronic Grisel’s syndrome has been treated with surgery. Many authors reported that patients with Grisel’s syndrome that remained unreduced for longer than 3 weeks are at a high risk of recurrence or permanent deformity, even after treatment, because of the development of chronic changes in the transverse and alar ligaments11,15). However, after surgical stabilization, continuing neurological complications happened up to 15% of all patients. Tetraplegia, limitation of bone growth, secondary deformity has been described1,9,14). Wright NM et al.17) described that C1-2 transarticular screw fixation, the risk of vertebral artery injury was 4.1% per patient or 2.2% for screw inserted and it rises to lateral medullary infarction, resulting in Wallenberg’s syndrome13). Because of its invasiveness and associated risk, we generally reserve the surgical option if the Grisel’s syndrome fails to resolve with non-operative care or there is a clear indication for surgery such as an associated traumatic spinal injury mandating surgical intervention6). There are many reports that chronic Grisel’s syndrome could be successfully reduced with antibiotic administration and observation for long periods of up to 6 month or with active physiotherapy7). Ishii et al.8) showed successful treatment of chronic rotatory subluxation (8 weeks) with traction and a sternal occipital mandibular immobilizer for 3 months. Park et al.11) described a case of chronic Grisel’s syndrome with 6 weeks of halter traction and 4 months of bracing.
The first acute Grisel’s syndrome case was successfully treated non-surgically. The chronic Grisel’s syndrome was also successfully treated with non-surgical management. Considering the patient’s age and potential for growth and development, we thought the surgery was too dangerous so that we performed conservative treatment for chronic Grisel’s syndrome patients. After 2 months of treatments, the alignment got corrected and symptoms improved.