INTRODUCTION
Spinal lesions can represent a broad spectrum of underlying infectious or neoplastic disease processes. As such lesions may indicate the presence of malignant tumors, physicians are required to make tissue diagnoses for said lesions6,17). A percutaneous biopsy is an important tool in the identification of metastatic tumors, primary tumors, and infectious spondylitis; further, this procedure is useful for confirming the presence of disease and collecting specimens to diagnose spinal tumors or infections1,5,13). Percutaneous bone biopsy is less invasive than an open biopsy, minimizes the risk of infection and wound-related complications, does not require general anesthesia, and has the advantage of being performed in an outpatient department.
Percutaneous bone biopsy using computed tomography (CT) and fluoroscopy guidance has been reported to be both effective and safe5,8,13,24). Its reported accuracy ranges from 16% to 100%14). However, it has been difficult to achieve accurate diagnoses when performing a percutaneous bone biopsy on sclerotic, cystic, osteoblastic, and osteolytic lesions because of its lower capacity to tear off the tissue9,28). Forceps are routinely used in gastrointestinal endoscopy and transbronchial biopsy2,18,21). However, to date, there have been few studies on the usefulness of using forceps for spinal bone biopsy. The purpose of this study was to demonstrate the safety and efficiency of performing a bone biopsy using forceps.
MATERIALS AND METHODS
This study was approved by the relevant Institutional Review Board (IRB) for human subjects’ research (IRB no. 2022-0130).
1. Patient Selection and Study Enrolment
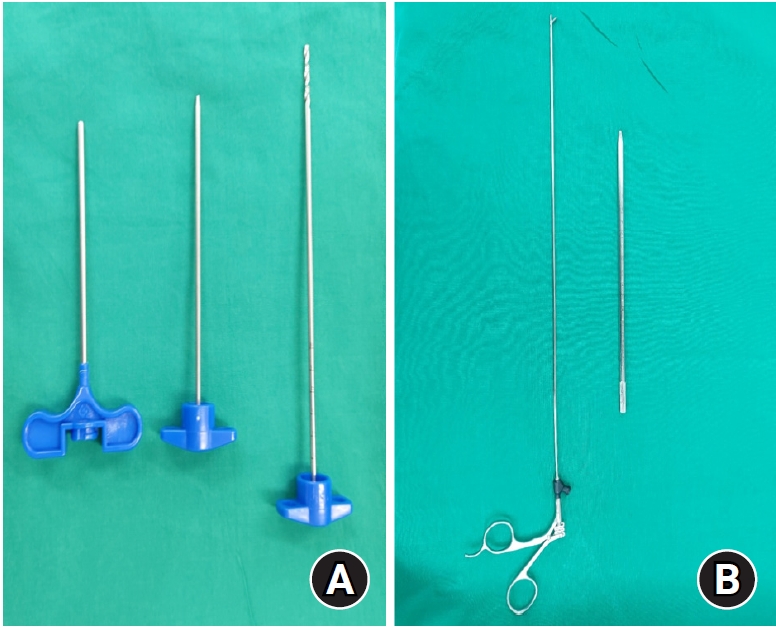
This multicenter (Seoul Asan Hospital, Gangneung Asan Hospital) retrospective study included patients who underwent fluoroscopy-guided spinal bone biopsy from July 2013 to November 2020 for suspected spondylitis, tumor metastasis, and primary tumor, as revealed on spinal CT and magnetic resonance imaging (MRI). For spondylitis patients, antibiotics were stopped 48 hr prior to the procedure28). When the biopsy diagnosis failed, open biopsy or surgery were performed. Alternatively, a re-biopsy was performed under consultation with the radiology department. Patients’ basic data such as age, sex, underlying diseases, intake of anticoagulants, bone mineral density (BMD), and smoking status were collected from the electronic medical record. Procedure-related factors such as instrument type, diagnostic yield, procedure time, and presence of specific lesions in the preoperative imaging were investigated. Spinal-specific lesions were identified as sclerotic, lytic, necrotic, or mixed, according to the bone matrix shown on CT before the biopsy procedure. Pain at the pathology site was assessed before and one day after the procedure, and was measured using a visual analogue scale (VAS). We divided participants into two groups according to the instrument used during the biopsy (a pair of flyer forceps [Wolf, Knittlingen, Germany] or a biopsy needle [Promega, Madison, WI, USA]) and analyzed all factors for both groups (Fig. 1).
2. Biopsy Procedure
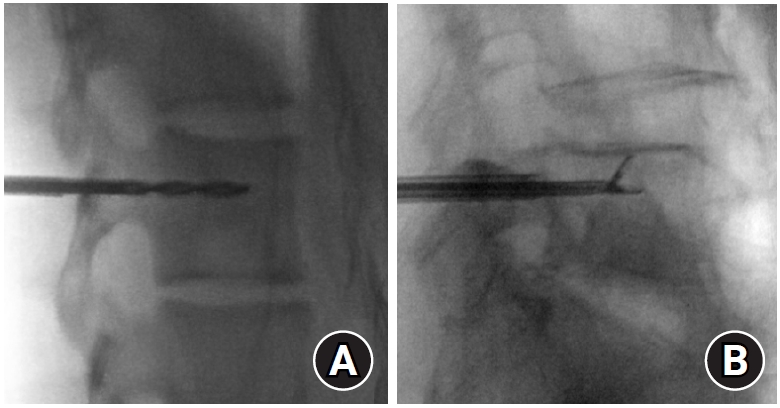
Consent was obtained after explaining the procedure’s potential complications such as nerve damage or hematoma to all candidates. All biopsies were performed by two specialists in spine biopsies. After reviewing the imaging findings, a biopsy tool (flyer forceps or a biopsy needle) was selected according to the operator's experience and preference. After the patient was placed in a prone position, a local anesthetic was infiltrated in a sterile state, and a skin incision was performed. To avoid injuring the nerves, the trocar catheter passed through the pedicle to approach the vertebral body, while fluoroscopic imaging was used to ensure the correct positioning of the trocar catheter. The biopsy instrument was placed in various parts of the lesion to allow for proper biopsy and bone biopsy was performed using a conventional biopsy needle or flyer forceps (Fig. 2).
3. Statistical Analysis
Data were presented as mean ± standard deviation values for the continuous variables and as absolute or relative frequencies for the categorical variables. Unpaired Student’s t-tests or Mann-Whitney U tests were used to compare the continuous variables, and χ2 tests or Fisher’s exact tests for the categorical variables. Statistical significance was set at p ≤ 0.05. All statistical analyses were performed using SPSS software for Windows (version 14.0; SPSS Inc., Chicago, IL, USA). All data were obtained from hospital charts and imaging study databases.
RESULTS
A total of 30 patients underwent spinal biopsy using a biopsy needle (n=16) or flyer forceps (n=14). The mean age was 59.43 ± 20.27 (range, 12-81 years). It was confirmed that both groups followed a normal distribution as a result of the normality test.
Bone biopsy was performed for 20 patients with metastatic tumors, three with sarcoma, and nine with infections. The diagnosis was unsuccessful in four patients. Of these, one patient underwent open biopsy, two underwent biopsy during surgery, and one underwent re-biopsy after consultation with radiologists. Serious complications such as nerve root and spinal cord injuries, hematomas pressing on the spinal cord, or wound infections were not observed.
There were no differences between the two groups in age, gender, underlying diseases, anticoagulant use, BMD, and smoking status (Table 1). Further, no differences in pain intensity (VAS score) before and one day after the procedure were observed between the two groups. In terms of operation time, shorter times were observed in the flyer forceps group compared with the biopsy needle group, and the difference was statistically significant (p=0.02). Regarding the accuracy of the diagnostic yield of the biopsy between the two groups, a higher value was observed in the flyer force group (100%), compared with the biopsy needle group (75%), and the difference was significant (p=0.04; Table 2).
1. Illustrative Cases
Case 1
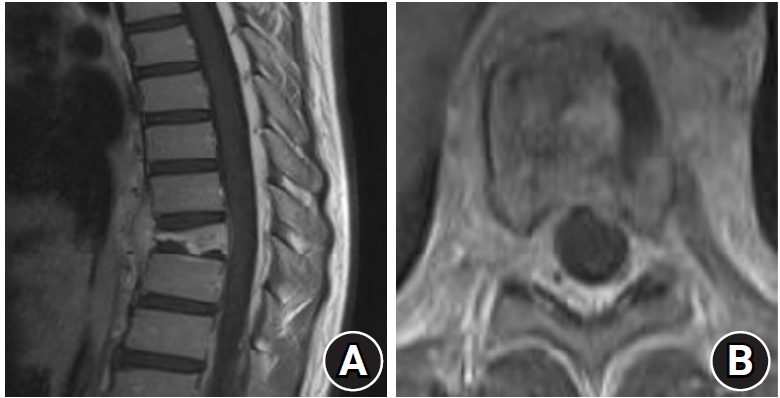
A 12-year-old female patient was admitted to our hospital after having developed back pain three months earlier. Her MRI showed a wedge-shaped compression fracture of the T9 vertebra. A T1-weighted enhanced MRI showed a highly enhanced T9 vertebral body, while an axial image showed vertebral body enhancement (Fig. 3). Although this patient had previously undergone CT-guided fine-needle biopsy at the radiological department, the collectors were unable to obtain a large enough specimen because of the small diameter of the biopsy needle. Subsequently, this patient was referred to our department. We also performed fluoroscopy-guided biopsy using flyer forceps. We were able to obtain enough specimens from the vertebral body. Some eosinophils in the fibrotic marrow space suggested the possibility of Langerhans cell histiocytosis. Thereafter, the patient was discharged one day after the biopsy. Observation without any further treatment except pain killers was determined and the patient’s status was good as of 40-months after the procedure.
Case 2
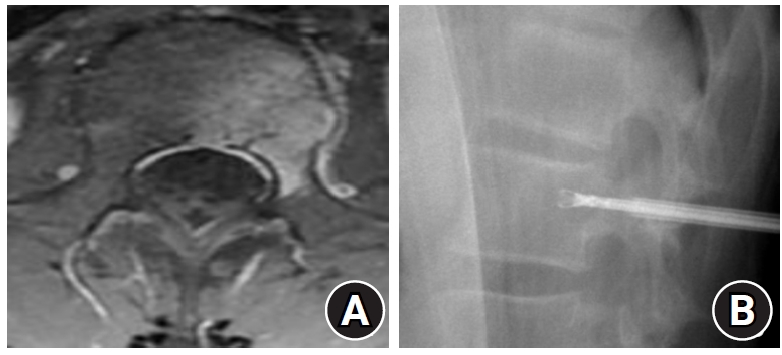
A 14-year-old male patient was admitted after complaining of back pain that had developed 9 months earlier. He had a history of acute B-lymphocyte leukemia at 9 years old. After chemotherapy, his leukemia was completely cured. Because of his newly-developed back pain, he underwent MRI. Subsequently, MRI showed left-side L1 vertebral body enhancement (Fig. 4). He had also previously undergone a CT-guided fine-needle biopsy at another hospital. Its result was also negative. After he was admitted to our hospital, we performed a fluoroscopy-guided biopsy through the pedicle using flyer forceps. We were able to obtain enough specimens from the vertebral body; multiple pieces of bone and fibrotic tissue were taken. The fibrotic tissue showed inflammatory cell infiltration with some CD1a-positive cells, and the final diagnosis was Langerhans cell histiocytosis. The patient was discharged one day after the biopsy. After histologic confirmation, observation without any further treatment except pain killers was determined. The patient’s status was good as of 3 months following the procedure.
DISCUSSION
This study examined the accuracy, safety, and usefulness of using flyer forceps for performing a bone biopsy, as opposed to using a biopsy needle. Unlike an open biopsy, a percutaneous needle biopsy provides a faster and more cost-effective approach with fewer complications5,15,27). Although the percutaneous bone biopsy has high diagnostic accuracy3,10,29) when the lesion is metastatic or recurrent sarcoma, the diagnostic yield is low for necrotic, cystic, or sclerotic lesions because it is ineffective to retrieve adequate specimens of the latter lesions7), and has a particularly poor capacity to culture infections4,11,12). In this study, diagnosis failed in 4 patients using a biopsy needle; an osteolytic lesion was observed in one patient, a sclerotic lesion was observed in one patient, and two were diagnosed with spondylitis (Table 3).
However, in the group in which the flyer forceps was used, three patients were diagnosed with sclerotic lesions, six with osteolytic lesions, and five with spondylitis, with 100% accuracy. Some of these patients also had a history of biopsy failure before visiting us. Additionally, there was no incident where the instrument was broken during the biopsy procedure (including sclerotic lesions).
However, several reports posit that a large needle (11 gauge [G]) is more useful to acquire adequate tissue for more accurate diagnoses25,28). The size is larger than the biopsy needle (13 G) and flyer forceps (2 mm diameter) used in this study. However, one study showed a potential for root injury, while another posited that a small gauge needle might be needed to sample lesions near critical structures22,26).
In the present study, two cases showed that the flyer forceps were effective even in children with small pedicles. In addition, it was confirmed that the flyer forceps group showed much shorter collection times than the biopsy needle group. The main reasons for failure in a spinal biopsy are fragmentation of the tissue and insufficient sample size3,30). However, sometimes the harvesting tissue becomes dry or damaged during storage before going to the pathology department. Surgeons planning to perform bone biopsy should also consider this aspect.
When the flyer forceps is used, a sufficient amount of tissue can be obtained in a relatively short time. Therefore, we believe that our method is not only accurate but also convenient. In addition, the discharge of all patients is possible one day after the procedure due to their rapid recovery and because no wound management is necessary.
The approach to the vertebral body comprises two main methods: a posterolateral approach and a transpedicular approach. In this study, only the transpedicular approach was implemented, as the posterolateral approach has a comparatively higher risk of complications such as hematoma, pneumothorax, and radicular pain5,8,20,24).
In addition, in this study, only fluoroscopy-guided biopsies were performed, while CT-guided biopsies were not. CT-guided biopsies have been confirmed to be safe and have high diagnostic accuracy in many studies16,19,23). However, fluoroscopy-guided biopsies have the considerable advantage of enabling real-time control of the position of the instrument, which makes them faster and cheaper, compared with CT-guided biopsies13).
Our study had four major limitations. First, logistic multivariate analysis could not be performed due to the small cohort. Second, selection bias occurred since the selection of instruments was determined by the patient's spinal bone lesions and clinical symptoms. Third, the biopsy needle used by each surgeon is different, and the operation time may vary depending on the type of biopsy needle, which may also act as a bias in this conclusion. Finally, the difference in the experience and skill of the two surgeons may have affected the results.
CONCLUSION
We have demonstrated the usefulness and safety of performing a bone biopsy using flyer forceps. The fluoroscopy-guided biopsy technique using flyer forceps allowed the effective collection of sufficient samples for all lesions (including osteolytic, necrotic, and sclerotic lesions) and more accurate diagnoses in relatively shorter times compared with biopsies performed using conventional biopsy needles.