INTRODUCTION
Hidradenocarcinoma is a malignant tumor that originates from the eccrine gland, and it has a very aggressive pattern. Local invasion and distant metastasis occur frequently, and the recurrence rate after treatment is also high1,3,6). So far, no standard treatment has been established because the incidence of hidradenocarcinoma is very low. The treatment option which most researchers have recommended is a complete resection2,13). Adjuvant treatment including radiotherapy and chemotherapy also can be tried, but the effectiveness of these treatment regimens is not clear.
CASE REPORT
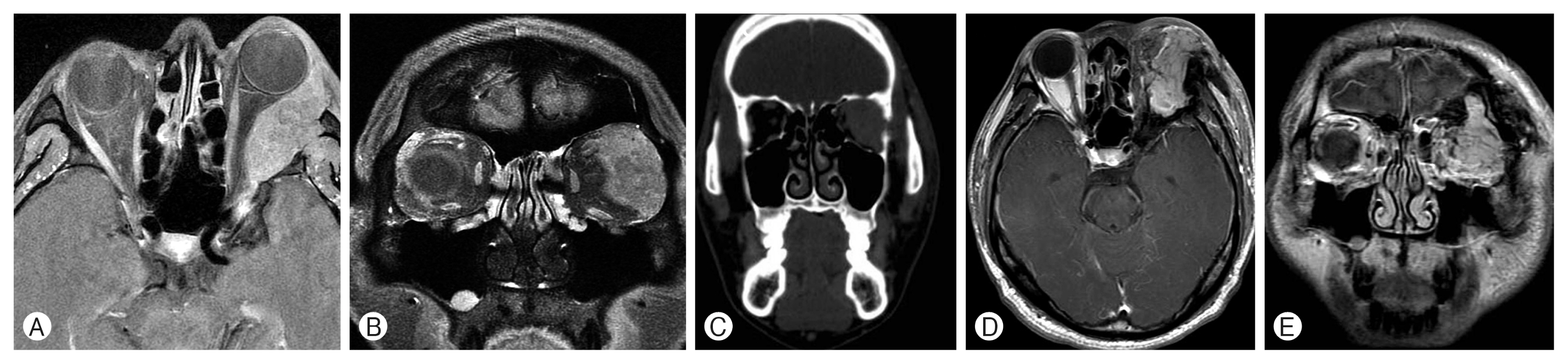
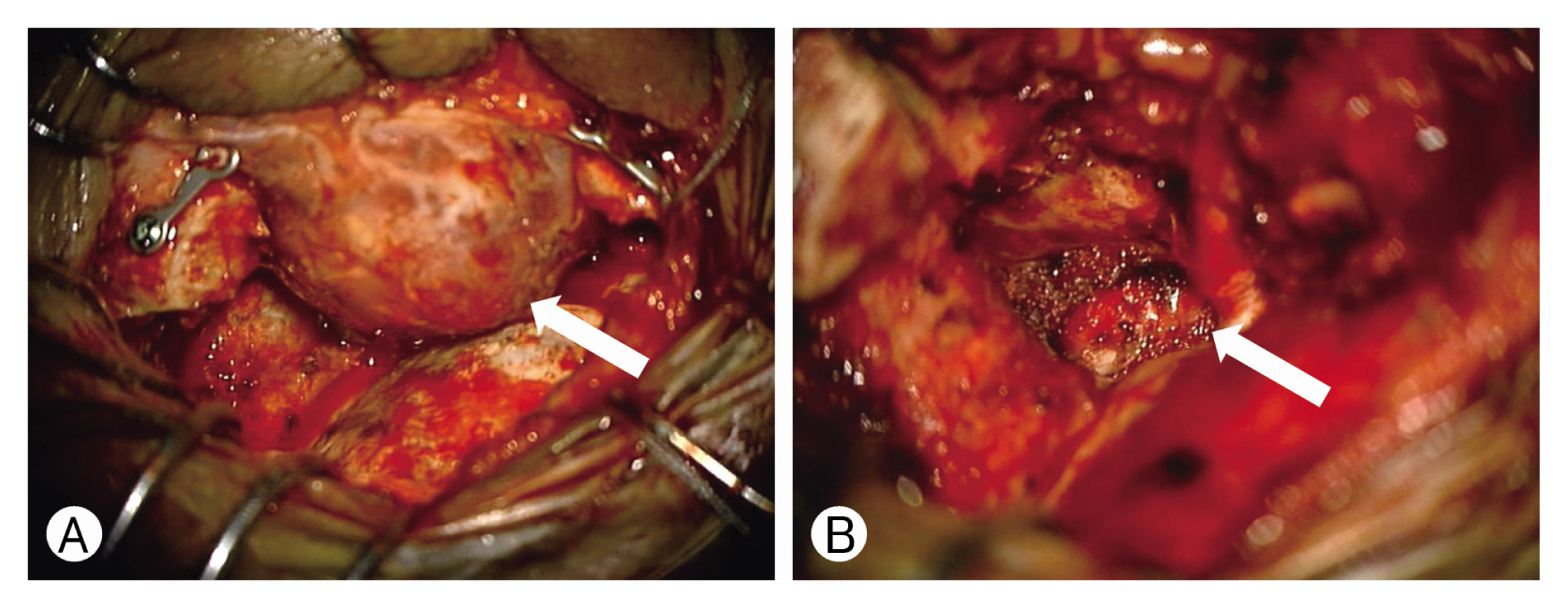
A 40-year old man presented with exophthalmus for 8 months and decreased vision for 1 month on left eye. The ophthalmological examination of left eye revealed visual field defect and decreased vision (0.2) and increased intraocular pressure (20 mmHg). Computed tomography (CT) showed a well enhancing tumor in the left orbit with focal bone destruction of lateral orbital wall and focal invasion into the anterior portion of left cavernous sinus. Magnetic resonance image (MRI) revealed a localized mass at lateral aspect of left orbit measuring 4.5×x 2.2×3.6cm3 in size which is iso-signal intensity on T1 and T2-weighted image, and heterogeneous enhancement at lateral aspect of left orbit. The focal bone destruction was seen at lateral orbital wall. The mass invaded into temporalis muscle, superior orbital fissure, and cavernous sinus (Fig. 1A-C). We performed a biopsy and the hidradenocarcinoma was diagnosed; hence, we planned to surgical resection with enucleation of eye ball. The grossly total resection was done through the modified lateral supraorbital approach (Fig. 2). The tumor appeared hyperemic and yellowish mass. Dissection the optic nerve from the tumor was difficult. The left eye ball was enucleated and fat packing was done. The immediate postoperative MRI showed no residual tumor.
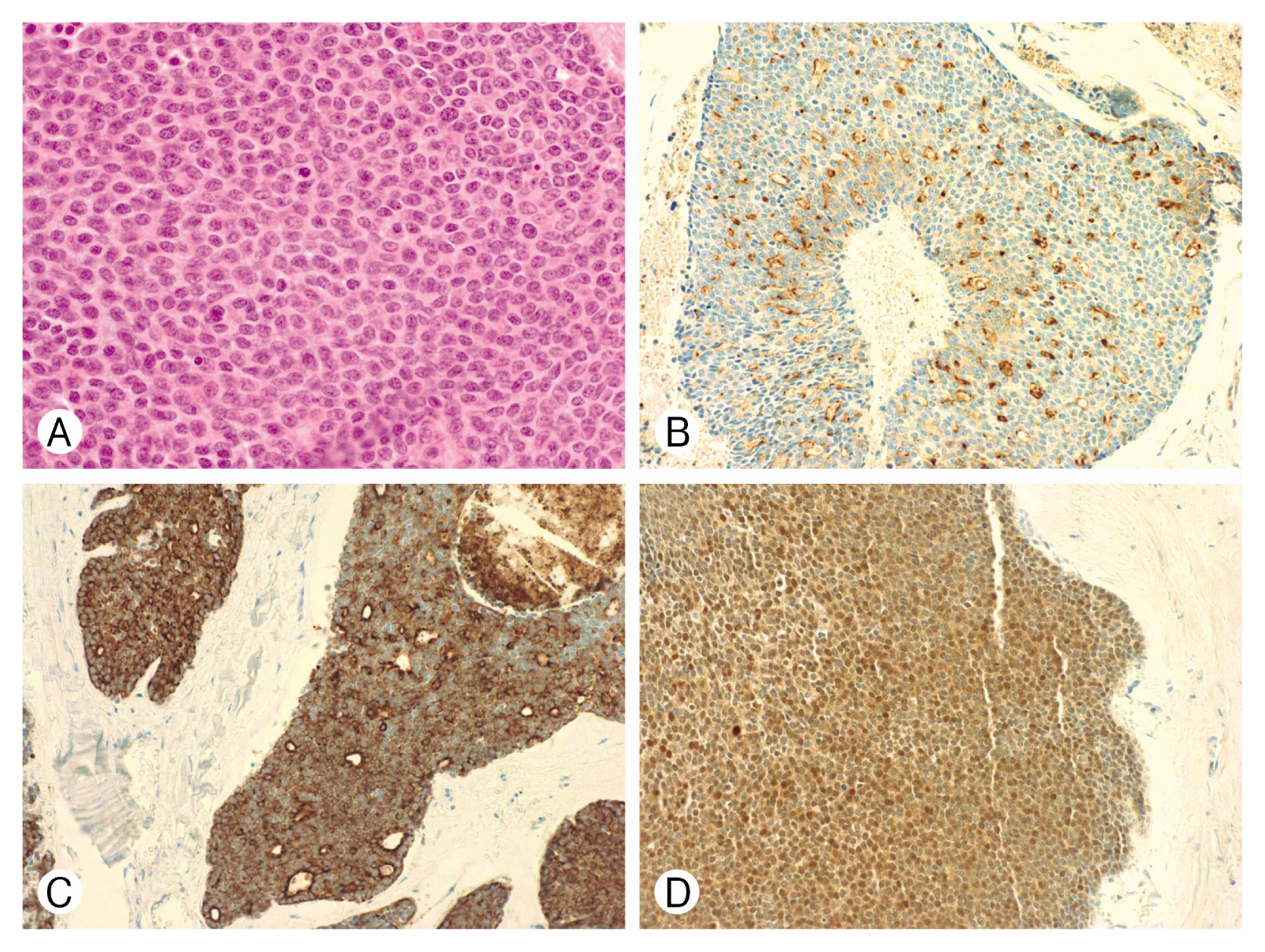
In the biopsy of the tissue removed by surgery, ill-defined multilobular tumors were extensively observed in dermis. The tumors were surrounded by pseudocapsules consisting with fibrotic stroma, and a cystic cavity caused by tumor necrosis was also observed. The tumor cells were round to polygonal in shape with a clear cytoplasm. Cellular atypia and mitosis were observed frequently. Additionally, we performed immunohistochemical staining, and the tumors were positive for epithelial membrane antigen (EMA), vimentin, cytokeratin, S-100, and high proliferation labeling index (Ki-67 30%), but they were negative for carcinoembryonic antigen (CEA) and gross cystic disease fluid protein 15 (GCDFP-15) (Fig. 3). Based on these histological findings and imaging study, we had diagnosed as hidradenocarcinoma on left upper eyelid extending into the left cavernous sinus with orbital bony destruction.
Considering the characteristics such as a very high recurrence rate and well metastasis of the tumor, adjuvant radiotherapy was performed with a total 5,400cGy/27 fraction. The patient’s status had been well maintained for 4 months without recurrence and complications.
The patient presented the sudden right eye visual symptom at 5 months after surgery. The ophthalmological examination of right eye revealed visual field defect and decreased vision (only light perception) and 16mmHg intraocular pressure. The mydriatic test result found a focal atrophy in the retina. In addition, the visual evoked potential result was that the P1 and P3 latency was delayed, and the electroretinography result found that the rod function was decreased. However, the multifocal electroretinogram was normal and both the MRI and positron emission tomography (PET)-CT image showed no recurrence and no metastasis (Fig. 4). We considered that the visual problem was associated with cancer associated retinopathy (CAR). And we started systemic steroid therapy and adjuvant chemotherapy. We administrated cisplatin and 5-fluorouracil. After the 1st cycle of chemotherapy, the patient’s cognitive function was getting worse and other cranial nerve (III, IV, VI) palsy was developed. We recommended the MRI evaluation and 2nd cycle of chemotherapy, but the patient refused the additional therapy. The patient expired at 7 month later.
DISCUSSION
Hidradenocarcinoma was first described by Keasbey and Hadley6) in 1954. It is a very rare tumor, and Keasbey found only 3 cases of hidradenocarcinoma among the 235 sweat gland tumors when he first described this tumor in 1954. Mehregan et al.11) mentioned that only 2 cases were diagnosed as hidradenocarcinoma among the 450,000 tissue samples collected for 20 years in the dermatopathology laboratory, and its prevalence is less than 0.001%6,11). So far, less than 70 cases have been reported. Patients with hidradenocarcinoma present with non-specific clinical symptoms. In most cases, a solitary cutaneous or subcutaneous lump for a long time period and the tumor size increases gradually. The tumor is often accompanied by ulcers, and occasionally there are a variety of clinical manifestations such as fleshy color or red to gray color. It may occur anywhere including the head, torso, legs, and arms; but, it mainly occurs on the head and neck according to the reports. Also most of the tumor shows rapid growth over weeks to months, and it can cause aggressive local invasion and metastasis to the surrounding lymph nodes or other distant organs1,3,5,6,14,16). In fact, hidradenocarcinoma has a poor prognosis, and the disease-free survival rate within 5 years is less than 30% according to the literature, and most of the reports suggested that distant metastasis is observed after tumor recurrence and eventually it leads to death8). Statistically, the local recurrence rate after surgical resection is approximately 50%, and more than 60% of the patients show metastasis to the lymph nodes, bones, skin, and internal organs13,15).
Hidradenocarcinoma is a histopathologically ill-defined multilobular solid tumor located from the dermis to the subcutaneous tissue, and tumor necrosis is often observed in the lobule. The polygonal-shaped cells have oval nuclei and clear to slightly eosinophilic cytoplasm. The tumor cells show significant nuclear atypia and moderate mitotic activity1,3,11). According to the literature, the immunohistochemical findings of hidradenocarcinoma are different, but most of the tumors are positive for vimentin, EMA, cytokeratin 5/6 (CK5/6), and they show various responses to S-100, Ki-67, and GCDFP-154,7,12). In this case, the tumor was microscopically diagnosed as hidradenocarcinoma which was positive for vimentin, EMA, CK5/6, S-100, and high proliferation labeling index (Ki-67 30%) and negative for GCDFP-15 and CEA.
No standard treatment has been established so far because hidradenocarcinoma has a very low incidence, and it is also challenging to treat the tumor due to its aggressive clinical characteristics. Wide resection is performed in most of the cases, and adjuvant therapy is considered as an additional treatment option. However, the prognosis of patients and clinical features still remain a matter of debate9,10,14-16). The wide local excision method may be a suitable local treatment option for non-disseminated lesions. However, although there is no evidence of distant metastasis and invasion of local lymph nodes on PET-CT, there is a possibility of microscopic invasion of lymph nodes in cases of locally aggressive invasion as in this case. Also, considering the high recurrence and metastatic rates of hidradenocarcinoma after surgery, we considered that combined treatment with wide excision and adjuvant radiotherapy would be appropriate for this patient. We performed adjuvant radiotherapy after complete surgical resection, and the patient is doing well and there has been no recurrence and complications for 4 months after surgery. However, 5 months after surgery, the patient’s opposite eye showed symptoms of CAR. We administered chemotherapy, but 7 months later the patient was dead. CAR is a rare phenomenon associated with existing malignant tumor, and there is no standard treatment guideline. Appearance of CAR can imply that there can be a remaining malignant cells. In the case CAR occurring in the patient’s opposite eye, we can consider that it would be a systemic metastasis.
We performed a gross total resection with postoperative radiotherapy and chemotherapy. And the patient was doing well for a relatively long time, considering the aggressive progression of hidradenocarcinoma. But, the disease progression was rapidly worsen after appearance of CAR. So, we considered that when hidradenocarcinoma is combined with cancer associated functional loss, it can act a poor prognosis factor.