INTRODUCTION
Spontaneous intracerebral hemorrhage (ICH) is one of the most serious complications that occur in patients with hypertension and atherosclerotic changes in blood vessels. Patients who diagnosed as ICH have a marked increase in blood pressure (BP) at the time of admission. Sustained increased BP in patients with ICH may lead to enlargement of the hematoma, so lowering BP is generally recommended in patients with acute ICH2,7,9,15,16).
However, there are studies that refute these treatments because excess lowering BP after onset of ICH can lead to cerebral ischemia as a result of lowering cerebral blood flow (CBF). Other studies have suggested that localized ischemia and acidosis in the ICH and surrounding areas may impair the intrinsic brain protective mechanism due to compression of the microvasculature, resulting in regional reductions in CBF and ischemia at the distant area of ICH. And, elevated BP can be a positive result of Cushing-Kocher reaction to keep cerebral perfusion, and if it is lowered, it could be an adverse role that interferes with the protective mechanisms of blood vessels itself3,5,6,8-10,17,18,21).
The imaging technique of perfusion computed tomography (CT) is useful to identify tissue hypoperfusion of surrounding the hematoma (penumbra), even though there was conflicting interpretation of ICH patients1,4,7,11,12,19,22).
Therefore, we investigated the effect of BP on perihematoma ischemia to provide a reasonable basis for nicardipine hydrochloride (HCl) therapy using a standardized BP management protocol in hypertensive ICH patients through this perfusion CT study.
MATERIALS AND METHODS
This study was performed in 32 patients in our single center, and the same protocol was applied as a standard practice in all practices. This protocol was introduced as a standard practice for review by the Institutional Review Board. During the study period, all clinical data were collected for acute ICH patients treated with nicardipine HCl protocol.
1. Patient Selection
The 32 patients included in this study were those who visited our single institution between January 2013 and December 2015 and were treated within 6 hr after the onset of symptoms. When the onset time was not described, the last time that was normal was regarded as the onset time. This study represents a continuous cohort.
Patient inclusion criteria were (1) no surgical hematoma removal was performed; (2) the patient with Glasgow coma scale is above 8; (3) The size of the hematoma measured by the formula of length×width×height/2 on CT is less than 60 mL11); (4) Patients with hypertension with systolic BP >140 mmHg at admission. Patients exclusion criteria were: (1) If they can not reliably assess the onset time or have a symptom before 24 hr; (2) fother intracranial lesions such as an aneurysm, arteriovenous malformation, or tumor; (3) hematoma in the cerebellum, brainstem or only in ventricles; (4) when taking medication that promotes a history of coagulopathy or congenital coagulopathy status.
And we collected information about the following risk factors: age, sex, previous diagnosed hypertension, diabetes, previous cerebrovascular attack, chronic kidney disease, any heart disease in each patient. This information was collected based on information from patients or family members or from previous medical records.
2. Treatment of Acute Hypertension Protocol
The treatment group’s BP target was to maintain systolic BP <140 mmHg and diastolic BP <100 mmHg within 24 hr of symptom onset. The initial treatment is as follows: nicardipine HCl was started intravenously at 10 mg/hr and increased to the maximum acceptable dose (15 mg/hr) by increasing 2.5 mg/hr every 15 min if target BP was not achieved. BP was monitored at the physician’s discretion using an intra-arterial catheter or non-invasive BP monitor. If the systolic BP drops under 110 mmHg, or diastolic BP drops under 70 mmHg, or if any symptoms due to hypotension are present, the antihypertensive treatment is discontinued and additional care is performed immediately by the physician.
3. Imaging Protocol
All patients underwent non-contrast CT immediately after visit to the emergency room for diagnosis.
If the patient was to be eligible, additional brain perfusion CT images were added, followed immediately by IV nicardipine, and brain perfusion CT images were taken again after 24 hr to discriminate the change of CBF on perihematoma region. The perfusion CT images were obtained by intravenous iodide contrast agent (40 mL) for more than 10 sec and CT images were collected for 50 sec (80 kVp, 200 mA per image) every 1 sec.
4. Measurement of Variables
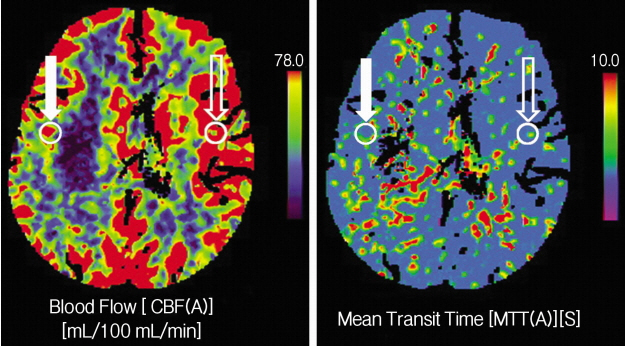
Raw contrast-enhanced CT images were transferred to a personal computer workstation and analyzed using a custom designed software package. Manual selection of a contralateral site of hematoma was used for correction of bolus delay and dispersion with a singular value of deconvolution algorithm. Quantitative perfusion maps including CBF were generated on a voxel-wise basis. From voxel-wise tissue impulse response curves, maximum oxygen extraction fraction (OEFmax) maps was designed based on transit time parameters. Arterial concentration of oxygen (CaO2) was estimated from arterial blood gas analysis from individual patients and the maximum cerebral metabolic rate of oxygen (CMRO2max) was derived from CBF ×OEFmax×CaO2 on a voxel-wise basis (Fig. 1).
5. Statistical Analysis
Statistical analysis was performed with t-test of linear mixed mode, Wilcox rank sum test and Fisher exact test. A p-value of 0.05 or less was considered to be statistically significant. Continuous variables were expressed as mean values and categorical variables were expressed as frequency.
RESULTS
A total of 32 patients were studied, 18 were men (56.3%) and 14 (43.8%) were women and their average age was 60 years (range, 25-84 years). Among the all subjects, 27 patients had a history of hypertension, a risk factor for ICH, was already diagnosed and the patient was taking medication. Other risk factor was diabetes (3), coronary heart disease (2), stroke (5), and end stage renal disease (1). Patients with coagulopathy, including platelet function, were excluded. On admission, the mean Glasgow coma scale was 12.9±1.1. ICH was mainly observed in typical locations (putamen 16, thalamus 13, lobar 3) and, in most cases, small-to-medium in volume (mean hemorrhage volume 19.3±11.6) (Table 1).
During the first 24 hr after admission, the BP of all patients was recorded hourly. Initial mean systolic and diastolic BPs were 176.8±15.6 mmHg and 94±13.9 mmHg, respectively.
Administration of nicardipine HCl by protocol reduced mean BP for the first 2 hr immediately after infusion, but did not show any decrease in BP until 24 hr. Mean systolic and diastolic BPs for 24 hr were 136.6±17.8 mmHg and 74.5±12.5 mmHg after injection, respectively (p<0.001, mixed effect linear model).
Initial CBF of affected perihematoma region was (51±8.3/100 g/min), and ipsilateral normal tissue CBF was slightly increased (43±12.8/100 g/min) and p-value was 0.32. After 24 hr continuous intravenous infusion of nicardipine HCl, CBF in normal tissues was slightly increased (46±9.5/100 g/min) compared to the that of admission, whereas affected CBF was slightly decreased (49±10.2/100 g/min), but p value did not show significant statistical difference.
In addition, the affected OEFmax (0.44±0.18) and the normal region (0.45±0.23) were almost the same at first, but after 24 hr, the affected OEFmax (0.43±0.36) showed slightly decreased data compared to the normal region (0.48±0.08) But did not show any statistically significant differences (p=0.71) Although the absolute value of OEFmax was slightly reduced, the oxygen supply to the tissue was within the normal range. The value of CMRO2max around the hematoma was also not different between the initial normal tissue and the affected tissue (3.29±1.55 mL/100g/min, 3.15±1.27 mL/100g/min; p= 0.76), and there was no significant difference between the two tissues after 24 hr (3.19±1.36 mL/100g/min vs. 3.28±2.08 mL/100g/min; p=0.82) (Table 2).
DISCUSSION
Treatment of acute hypertension in patients with hypertensive ICH - to what extent it is necessary to lower BP is still controversial. The persistent severe acute hypertension (>200 mm/Hg) may cause abrupt elevation of cerebral perfusion pressure (CPP), which may increase the size of the existing hematoma and exacerbate the edema, intracranial pressure (ICP) leading to cerebral ischemia.
However, on the other hand, a rapid drop in BP that causes loss of autoregulatory mechanisms around the hematoma can reduce CBF in and around the ICH, resulting in ischemia and cerebral perfusion failure5,6,8,10,17,21). Due to the ability of the autoregulation to maintain CBF as a change in diameter of the arteriole relative to changes in CPP, changes in BP within the normal range have little or no effect on CBF.
Under normal circumstances, the relationship between ICP and CPP can be maintained with autoregulatory mechanism. CBF will return to normal range within a few sec because there is vasodilatation of cerebral resistance vessels, decrease in cerebrovascular resistance and increase in cerebral blood volume as the CPP falls within the autoregulation range. However, if this condition persists, the autoregulation ability will not work and eventually causes a decrease in CBF, resulting in ischemia3,5,6,8-10,17,18,21).
Previous studies have demonstrated an early phase of reduction process of CBF around ICH. The initial decrease in CBF immediately after ICH appears to reflect the immediate and hemodynamic reaction, and a raised ICP was observed as a compensatory mechanism that makes CBF normal13,20,21). Nath et al.13) showed 10 min of ischemia immediately after ICH and showed recovery of CBF to normal within 3 hr. Similarly, Yang et al.20) confirmed that CBF with ICH reduced by 50% returned to normal after 4 hr.
Powers et al.14) reported that 14 ICH patients with nicardipine infusion using a positron emission tomographic scan showed no effect on CBF of perihematoma area and ipsilateral normal region, while decrease in mean arterial pressure about 17% from baseline. In general, previous studies suggest that changes in CBF after a decrease in mean BP are not consistent with ICH because self-regulation is maintained after ICH1,5,13,21). We have not found any negative effects of reducing mean perfusion over a 24-hr period and no evidence of ischemia was found in any patient. The results of our study are consistent with previous studies mentioned above. Decreased cerebral vascular resistance by nicardipine causes compensatory vasodilation, suggesting that CBF is maintained. This suggests that the controlled use of nicardipine HCl after ICH significantly reduces the mean BP, meaning that CBF, OEF, CMRO2 is maintained simultaneously.
There are some limitations in our studies. First, patients with a hematoma volume less than 60 mL and patients with good Glasgow Coma Scale were selected. In patients with larger amount of ICH, a higher ICP is induced, which requires a rapid increase in systemic BP and a sudden change in autoregulation. Relatively, patients with smaller hematoma investigated in our study have lesser changes in ICP, so the effect of nicardipine on changes in CBF may be compensable, but it is difficult to assume that blood flow is still maintained even in large hematomas because we did not measure the ICP of patients directly. Second, this study of a relatively small number of patients (32 patients) is not sufficient to conclude definitively. Third, the existence of unknown, confusing variables not explained in the final analysis can not be ruled out. The possibility that dynamic cerebral autoregulation has already been impaired by an already existing vascular risk factor such as chronic hypertension, diabetes and silent infarction can not be ruled out.
CONCLUSION
This study supports the controlled use of nicardipine HCl for acute phase ICH based on no significant changes in perfusion around the ICH with a meaningful decrease in mean BP. If the reduction in BP affects CBF, OEF, and CMRO2, requiring more research based on large, well-designed, randomized, controlled, and long-term outcomes. Our study can help to design such trials and can provide useful guidance when lowering BP is needed in patients with ICH.