CASE REPORT
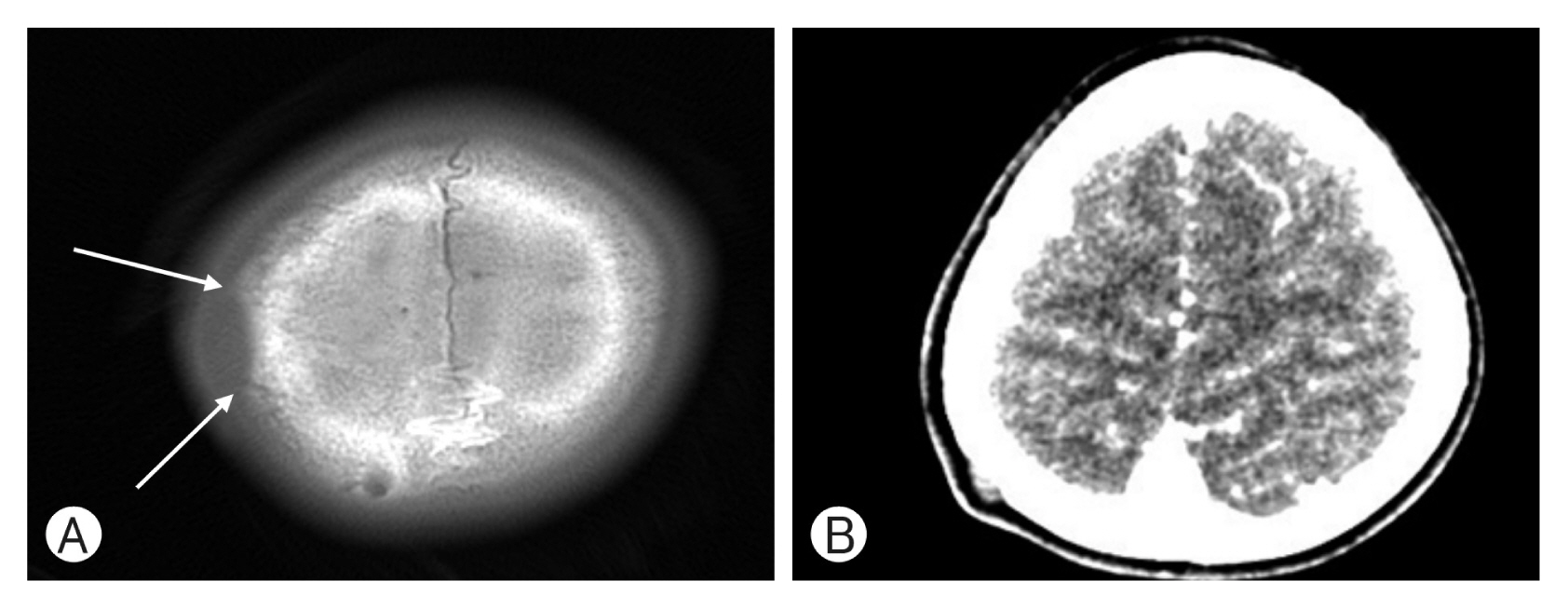
A 6-year-old right-handed female child presented with skull depression which was detected by her mother. She reported previous intermittent episodes of headaches within the past month. She had no significant medical or surgical history and her general and physical examination was normal. An initial work-up of the patient included a brain computed tomography (CT) scan, which revealed a ovoid bone defect due to extrinsic compression by soft tissue mass at right parietal bone (1.0×0.4 cm; Fig. 1). This lesion was not without intracranial extension or associated brain abnormality. Possible preoperative diagnosis was interpreted as an underlying epidermal inclusion cyst or small low flow vascular malformation such as lymphangioma. Brain magnetic resonance image (MRI) showed a lesion of signal abnormality on the right parietal bone with indentation to adjacent bone. On unenhanced T1 image, this area exhibited low signal intensity, and high signal intensity on the T2-weighted images with no enhancement on the post contrast images. On the coronal images, there was no intracranial extension or associated brain abnormality. Note was made of erosion of the overlying cranial vault (Fig. 2).
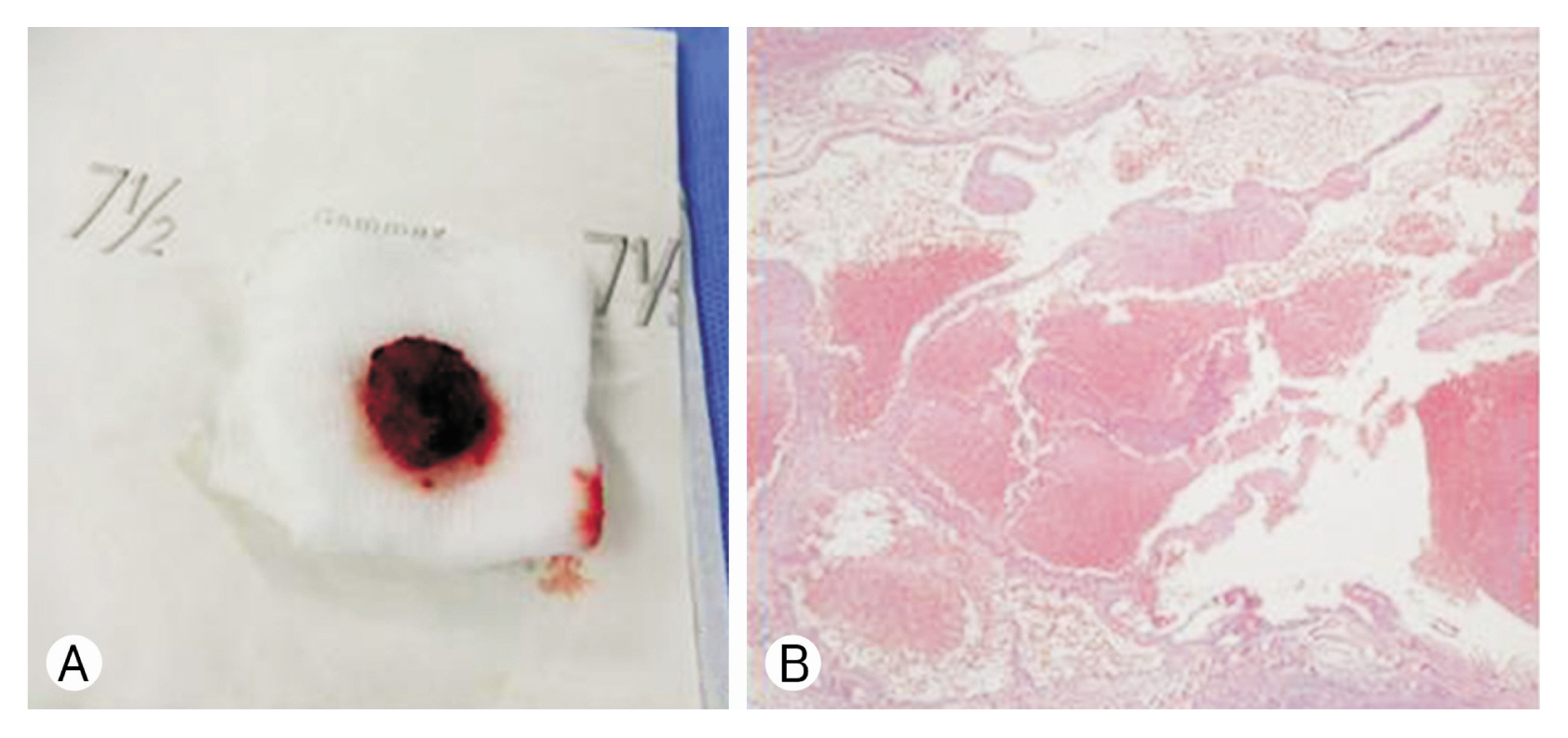
She was treated by operation with total excision of mass followed by a cranioplasty. At operation, abnormal soft tissue was noted in the right parietal bone defect with the presence of hemorrhagic tissue (Fig. 3A). The lesion and bone were removed all the way along with 0.5 cm of normal bone margin. Pathologic examination of the lesion and bone revealed a capillary hemangioma consisting of thin-walled blood vessels, some of which were distended with blood. The hemangioma invaded the bone which showed some reactive osteoblastic activity with new bone formation (Fig. 3B). She recovered to a favorable state without any neurological deficit.
DISCUSSION
CH in cranial vault, are rare benign tumors of blood vessels, more commonly found in the spinal vertebral column. Overall, they represent less than 1% of all osseous benign tumors1-3,5,6,8-10). The parietal bone is thought to be the most commonly affected, followed by the frontal bone and less frequently by occipital and temporal bones. They are usually solitary. CH in cranial vault, are slow-growing lesions and typically occur in women in the second through fourth decades. Only less than 10% of cases are observed during the first decade as in our cases1-3,5,6,8-10). The natural history of untreated lesions is poorly described. Cosmetic alterations, bleeding, and cranial nerves with progressive involvement in tumors of the skull base, as well as progressive exophthalmia and impairment of ocular movements in orbital lesions, were reported in some cases1,2,5-10). The symptoms are usually pain and visible or palpable bony hard mass or skull defect, slowly growing, covered by normal skin. Neurological deficits are unusual because these tumors tend to expand externally, but intracranial expansion has been reported8,9). Radiography of the cranial vault is the most useful method to identify intraosseous CH as an intradiploic, well-circumscribed radiolucent rounded lesions with a partially sclerotic margins and sunburst or honeycomb pattern of trabeculations and protrusion into the external plate of skull. These characteristics are better defined on CT scan, which revealed an intradiploic hypodense lesion with rarefaction. The CT scan is more helpful than MRI in planning surgery because it shows the location and extent of tumor better in bone windows. The signal characteristics on MRI are variable. The lesion usually appears mottled and heterogeneous with both increased and decreased signal intensities on both T1- and T2-weighted images. The signal depends on the quantity of slow-moving venous blood and on the ratio of red marrow to converted fatty marrow present within the lesion. CH typically enhance after administration of gadolinium. High signal intensity on T2-weighted MRI may be caused by pooling of blood or slow-flowing blood. In angiographic examination, most of CH lacks a vascular blush, and diagnosis of hemangioma may not be suggested1-6,8-10).
CH are composed of group of large, dilated blood vessels separated by fibrous tissue, whereas capillary hemangiomas lack fibrous septa and have smaller vascular lumens. Most of the CH in cranial vault are of the cavernous type, whereas vertebral CH are most frequently of the capillary type. They are supplied by branches of external carotid artery (middle meningeal artery and superficial temporal artery), arising in the cranial vaults. The bony trabecula seen within this tumor is believed to be the result of osteoclastic remodeling and osteoblastic reinforcement by the growing vascular tumor1-10).
The differential diagnosis includes osteoma, osteoblastoma, aneurysmal bone cyst, giant cell tumor, fibrous dysplasia, sarcoma, meningioma, metastatic disease, Paget disease, dermoid and epidermoid cyst. These tumors are not difficult to identify by epidemiological, clinical and neuroimaging methods, but the frequent atypical or small cases are not so easy to differentiate1-3,5,6,8-10). Radiating lattice-like or web-like trabecular pattern of the skull by bony erosion may be seen in radiographs in cranial vault CH. The osteoclastic activity of the tumor and following osteoblastic remodeling with trabecular bone result in the “sunburst” appearance on radiograph1). Osteosarcoma can also present osteolytic lesion but it involves both inner and outer table. Histopathologic confirmation can be effective for making definite diagnosis.
The current treatment of choice for CH in cranial vault is surgical monobloc resection. To prevent recurrence, removal of the lesion plus a wide margin of uninvolved normal bone is always recommended. This method removes the tumor intact and remains the standard approach. Embolization of tumor before surgery is helpful in preventing excessive bleeding1-3,5,6,8-10). Recurrence of CH suggests that lesions develop from vasculature that is present already in response to a proliferative stimulus. Reconstruction of the cranial vault defect with methyl methacrylate often made favorable cosmetic results. The other therapeutic options for these tumors are curettage and radiation therapy1-3,5,6,8-10). Curettage canal so involve excessive blood loss and disturbance of hemostasis, and carries a higher risk of recurrence than surgical excision. Radiation therapy may stop tumor growth but does not reduce the size of the tumor and has a risk of development of malignant transformation. The radiation therapy has a role in lesions that are felt to be unresectable or residual tumors from subtotal resections, such as those that deeply invade the bone, orbit, or cavernous sinus.