INTRODUCTION
Compressive radial neuropathy, a type of nerve entrapment, can cause pain, extensor weakness, and sensory change5). The diagnosis and subclassification are largely based on clinical features, especially the patient’s chief complaint. When pain in the forearm, specifically in the region innervated by radial nerve, is the patient’s only symptom, clinicians give a diagnosis of radial tunnel syndrome (RTS). In contrast, when motor weakness from the weakened muscles governed by the radial nerve is the main symptom, posterior interosseous nerve (PIN) syndrome is considered a diagnosis. In the following case, the patient complains of both pain and motor weakness of forearm6). Therefore, in the traditional way, the subject had both RTS and PIN syndrome. We present our experience of alleviation of both symptoms after surgery and suggest that the choice of treatment should be based on symptoms and mechanism as a diagnostic process, rather than the classification of syndromes. Additionally, for patients with radial neuropathy (RTS) whose symptoms, especially motor weakness, are refractory despite conservative treatment, i.e. steroid, we suggest timely surgical intervention as an effective treatment modality that leads to a better outcome. We present the following case in accordance with the CARE guidelines.
CASE REPORT
A 58-year-old male patient was referred to us by a local clinic. The patient complained of difficulty using his right hand properly and intractable pain in his right forearm. Pain in the posterior forearm started about 6 months ago. In addition, wrist and finger drop appeared suddenly 2 months later. He first tried treatment for herniated cervical disc disorder, which resulted in no improvement. He was a farmer with no underlying disease and had no history of trauma to his right arm.
1. Physical Examination
Tenderness of the posterior forearm, especially between the brachioradialis (BR) and the extensor carpi radialis brevis (ECRB) was noted. He showed right-sided motor weakness in wrist extension (grade 4), finger extension (grade 3), and supination (grade 4). This suggested radial nerve neuropathy. The patient also showed a radial shift during wrist extension, suggesting that extensor carpi radialis longus (ECRL) function was intact, and the affected lesion was located more distally from the elbow joint. Paresthesia was also present in his lateral proximal forearm, dorsum of the hand, and the 3rd digit, largely corresponding to the region innervated by the radial nerve.
2. Diagnostic Imaging
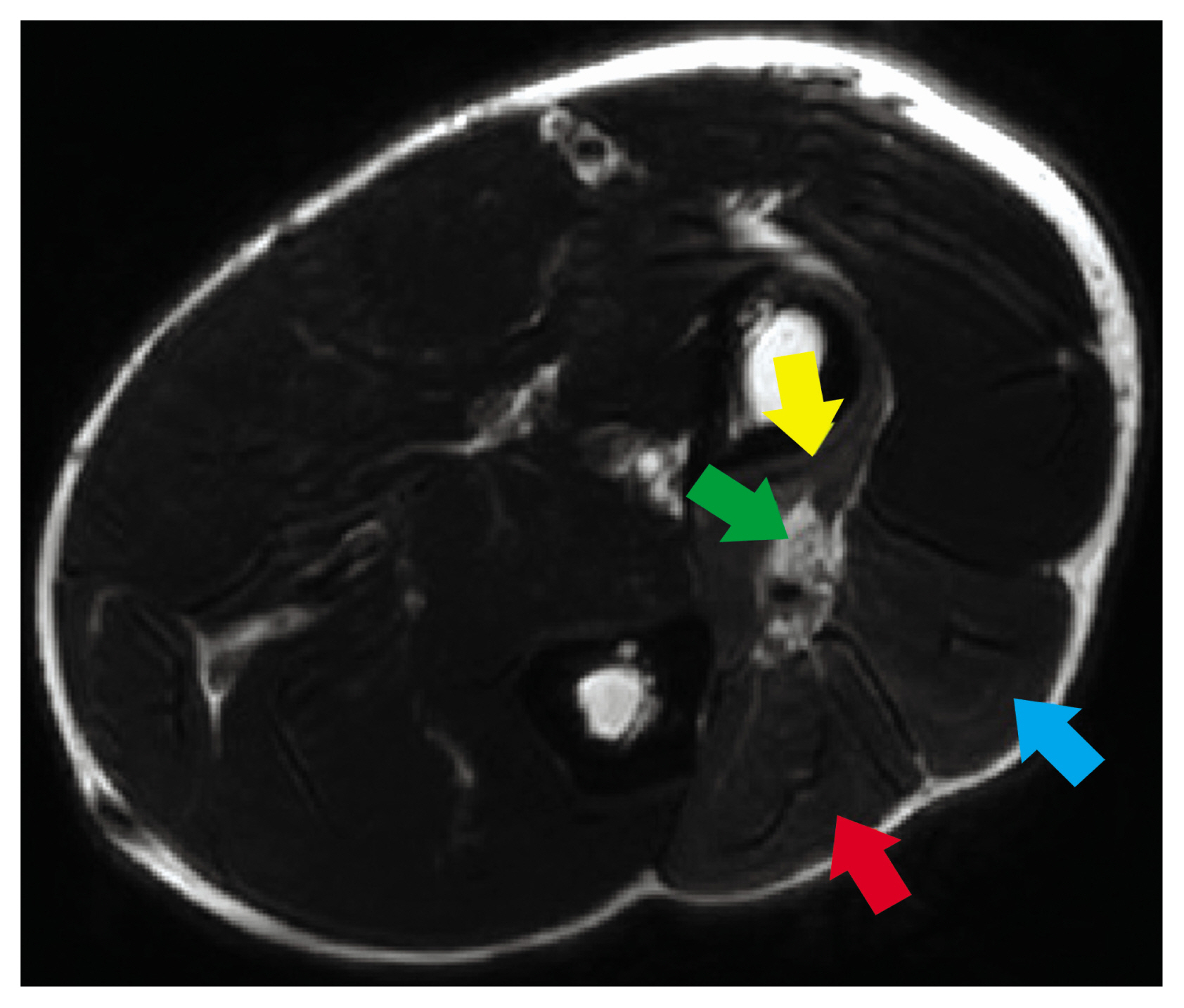
Magnetic resonance Imaging (MRI) showed abnormal enlargement and high T2 signal intensity in the patient’s right radial nerve from his elbow joint extending to the PIN (Fig. 1). Muscle edema was also noted at the supinator, the extensor carpi ulnaris, the extensor digiti minimi, and the extensor digitorum communis. These findings were consistent with compressive radial neuropathy, affecting the nerve within the radial tunnel.
3. Surgical Approach
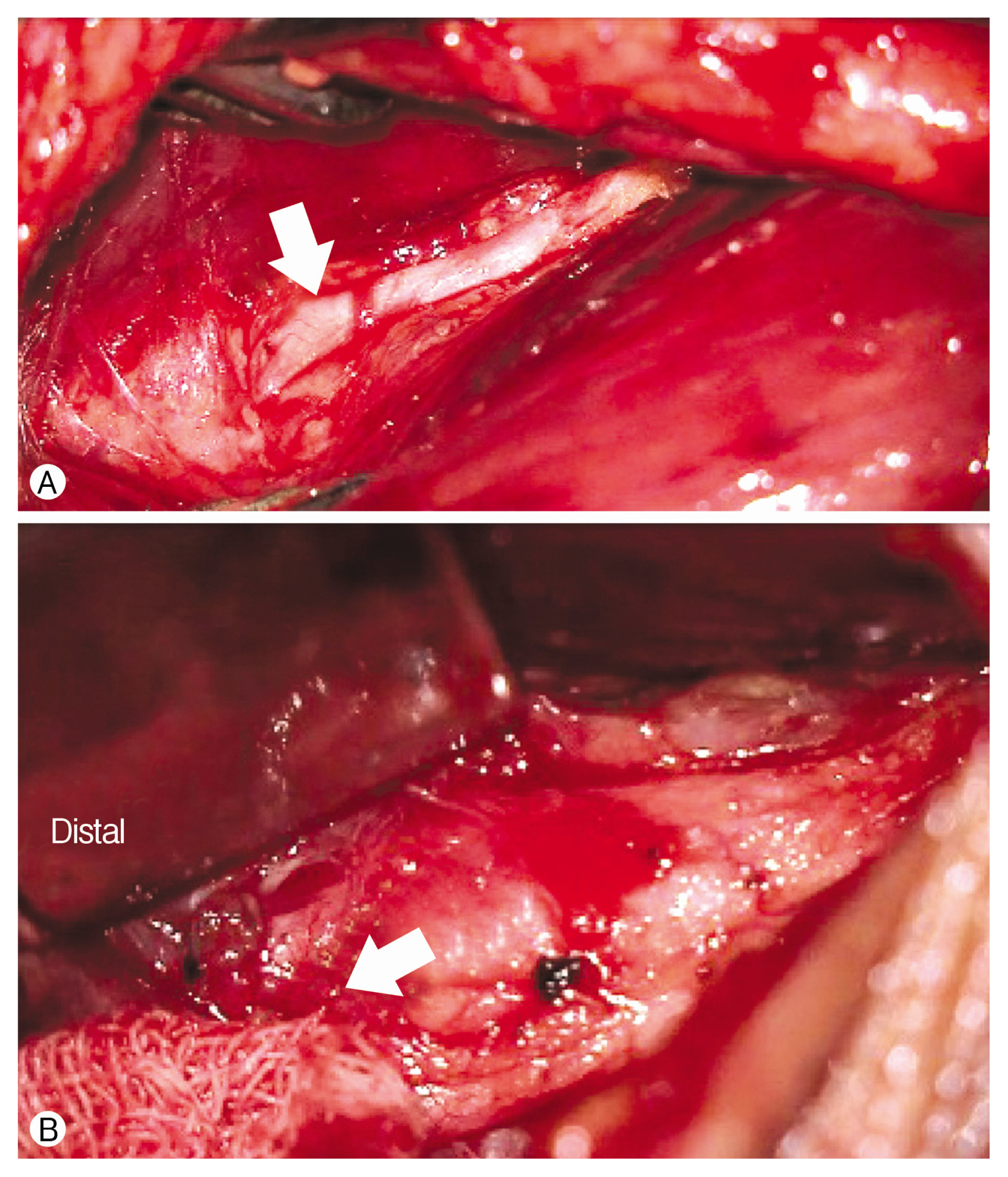
Under general anesthesia, we made a lazy-S incision between the BR and the ECRB. Retracting the BR showed compression of the superficial radial nerve (SRN), and surrounding adhesions were noted (Fig. 2A). After performing adhesiolysis, we explored proximally to expose the bifurcation of the SRN and the PIN, removing adhesions along the course. The PIN was severely compressed and pale-looking, so while following its course distally from the bifurcation, we tried to remove as much tissue as possible to get adequate decompression. The PIN appeared compressed at the arcade of Frohse as well (Fig. 2B), and after external neurolysis and decompression, we confirmed that the radial nerve and its branches were properly decompressed. The patient experienced no perioperative complications.
4. Outcome
Two weeks after surgery, his motor weakness improved from grade 4 to grade 4+, and his pain disappeared. At the 1-month follow-up, his motor function of the forearm had returned to normal strength. Normal muscle tone in the innervated radial nerve was retained until his 3-month follow-up.
DISCUSSION
The radial nerve, extending from the posterior cord of brachial plexus, coursing through the spiral groove of the humerus to the forearm, passes a structure called the radial tunnel, then divides into 2 branches. This tunnel is bound by the BR, the ECRL and the ECRB laterally, and the tendon of the biceps brachii and the brachialis medially. The aforementioned nerve branches are: SRN, receiving sensory information from the posterior forearm, the dorsum of hand, and the dorsal aspect of the 1st, 2nd, 3rd, and lateral side of the 4th digits; the PIN mainly providing extensor motor function to the forearm1).
During its course, the radial nerve, especially the PIN, the deep motor branch of the radial nerve, can be compressed by one of the following structures: fibrous band tissue between the brachialis and the BR, recurrent radial vessels (or leash of Henry), the fibrous arch of the ECRB, proximal and distal fibrous arches of the supinator. Among them, a fibrous arch at the proximal end of the supinator, also known as an arcade of Frohse, is the most common structure causing compressive neuropathy6).
As mentioned above, a distinction is usually drawn between PIN syndrome in which weak extensor function is the main symptom and RTS causing pain but no motor weaknesses3). PIN syndrome is relatively considered an objectively evaluable disease, compared to RTS. Furthermore, RTS is considered a less well-known and controversial disease entity. This is partly due to the lack of electrodiagnostic proof of the existence and severity3). Another possible reason for controversy is the inability to demonstrate the pathology. Unlike the suggestion of some that irritated PIN causes RTS3), it is almost always impossible to demonstrate the corresponding irritant in the surgical field6).
In our case, decompressing the PIN and the SRN from adjacent adhesion tissues resulted in the relief of both pain and motor weakness. The symptom improvement of PIN syndrome from surgery is relatively explainable and is in alignment with various other studies. The theory for alleviation of RTS is 2-fold. First, as pointed out in previous studies, freeing the PIN from adhesion tissues resulted in the absence of pain. Second, decompressing the SRN may have resulted in pain relief. The most well-known form of SRN compression, Wartenberg’s syndrome, presents as a painful sensation in the region innervated by the SRN. The differences between RTS and Wartenberg’s syndrome are the regions affected and the compressed location of the radial nerve. In Wartenberg’s syndrome, SRN in the middle forearm is affected2), whereas in RTS, just as our patient’s case, the radial nerve is compressed at the bifurcation of the radial nerve. Although the compressed location was different, maybe the patient experienced symptom relief from surgical decompression of the SRN just as a patient with Wartenberg’s syndrome experiences improvement after surgery4).
One thing to point out is that the choice of treatment should largely be based upon the patient’s clinical presentation and the mechanism of symptom development. If our patient did not experience motor impairment symptoms, as surgery in RTS still lacks clinical evidence, he would not have had a chance to get total pain relief6). Localizing the lesion led us to perform the best possible treatment for the patient and resulted in clinical improvement. Subclassifying the patient’s disease would not have been helpful in the process.
CONCLUSION
In the diagnosis of compressive radial neuropathy, neurologic examination is crucial, and MRI would be helpful for confirmation. If the patient’s symptoms do not improve with conservative management, surgical decompression, and external neurolysis of the radial nerve may result in a favorable outcome.