INTRODUCTION
Cervical radiculopathy is caused by mechanical compression and subsequent inflammation of a cervical nerve root. Common causes of the condition include soft disc herniation, neural foraminal stenosis by an osteophyte, ossification of the posterior longitudinal ligament, or traumatic fracture, but rare conditions like neoplasia also need to be considered4,19).
Melorheostosis is a rare connective tissue disease that causes overgrowth of cortical bone16,20). The condition is also called as Léri disease after it was first described by Léri and Joanny9) in 1922. Although more than 400 cases of melorheostosis have been reported in the literature, isolated spinal involvement requiring surgery is extremely rare15). In addition, the only 2 case reports of melorheostosis involving the cervical spine manifested with myelopathy, rather than radiculopathy, due to thecal sac compression. To the best of our knowledge, no case report has been issued on isolated cervical radiculopathy caused by melorheostosis in the absence of myelopathy.
CASE REPORT
1. History
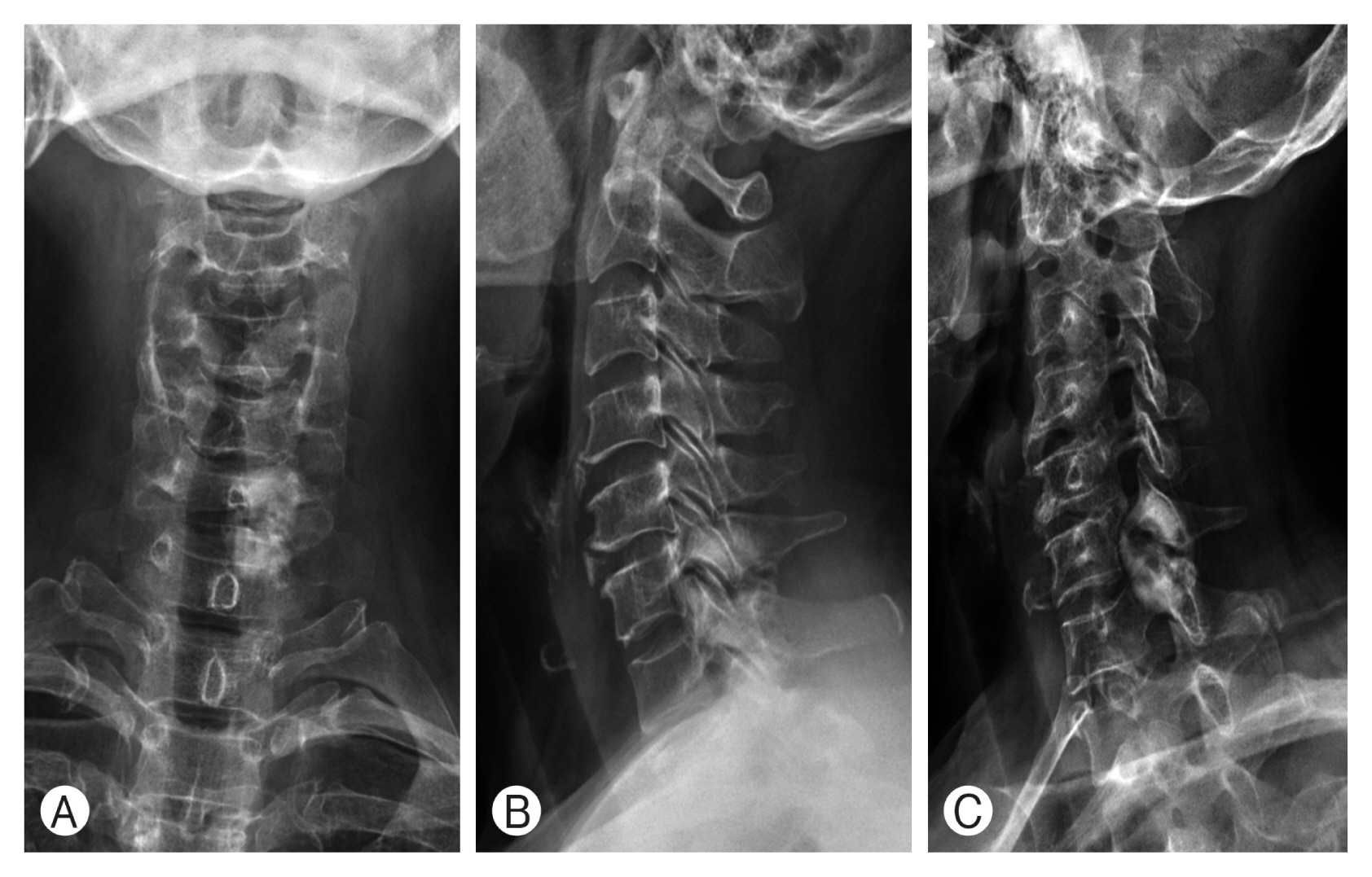
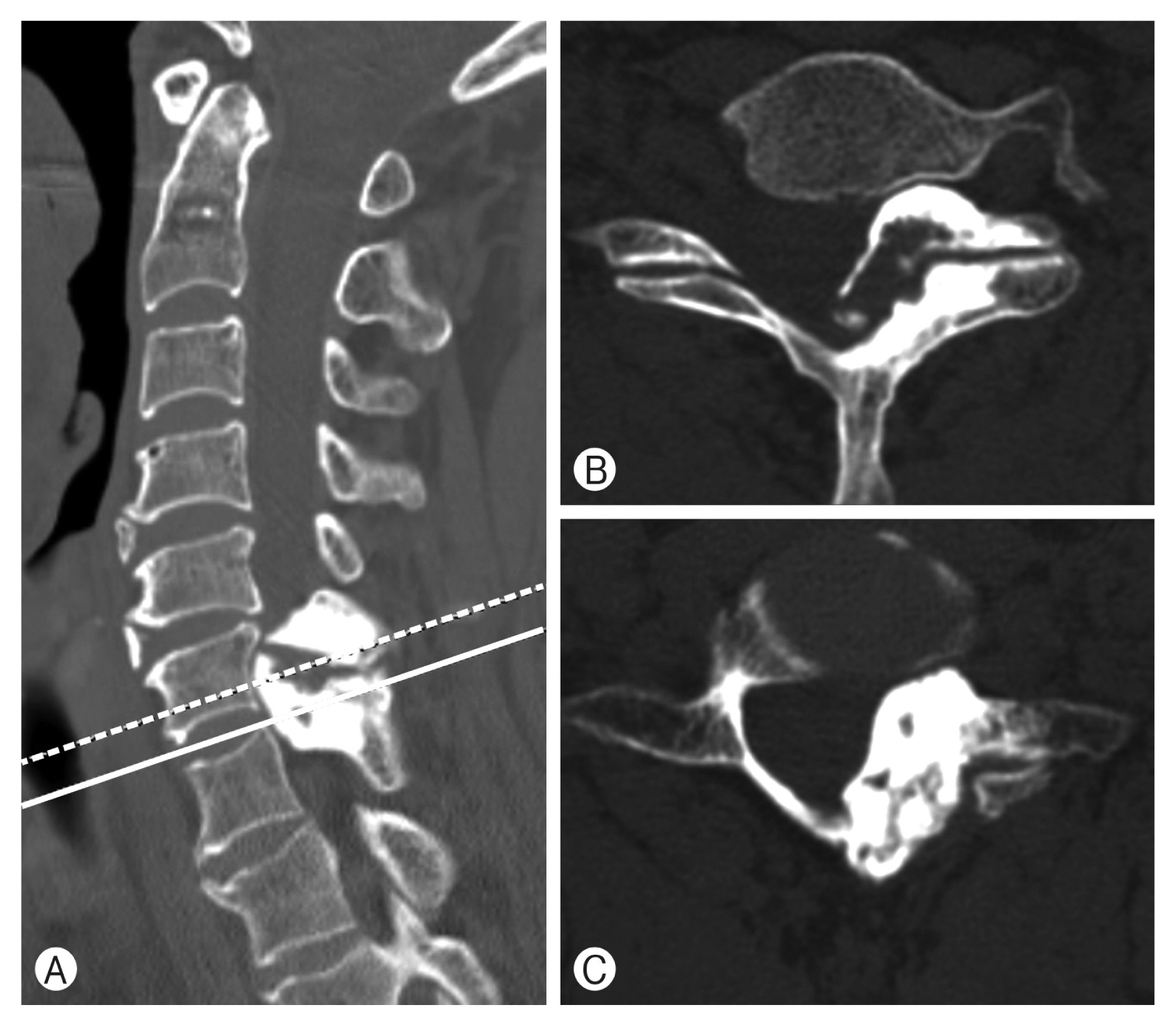
A 59-year-old woman visited our outpatient clinic with persistent neck pain and radiating pain to the left arm of 3 months duration. The patient described a continuous tingling sensation and numbness along the neck, left shoulder, outer part of the left upper arm, dorsal aspect of the forearm, and dorsal area of the middle finger consistent with C7 nerve root involvement. There was no history of previous medical disease. The patient had tried non-steroidal anti-inflammatory drugs, muscle relaxants, and physical therapy but without any improvement in symptoms. Her physician at a local clinic referred her to our institute for surgical treatment under a tentative diagnosis of bone tumor. Neurological examination revealed left C7 dermatomal hypoesthesia but intact motor functions. Laboratory tests at admission were normal. A plain radiograph of the cervical spine showed hyperostosis involving the left facet joint at C6/7. Computed tomography (CT) and magnetic resonance imaging (MRI) of the cervical spine revealed hyperostosis extending into the central canal, inlet portion of the left neural foramen of C6/7, and almost to the posterior surfaces of C6 and C7 vertebral bodies that resulted in a right side deviation of the spinal cord and severe neural foraminal compromise on the left side of C6/7. Pressure erosion into the left posterior surface of C6, 7 vertebral bodies was also observed (Fig. 1-3). A whole-body bone scan demonstrated increased uptake in L3 but an additional CT scan of the lumbar spine showed thickening of vertebral trabeculation in the L3 vertebral body suggesting intraosseous hemangioma.
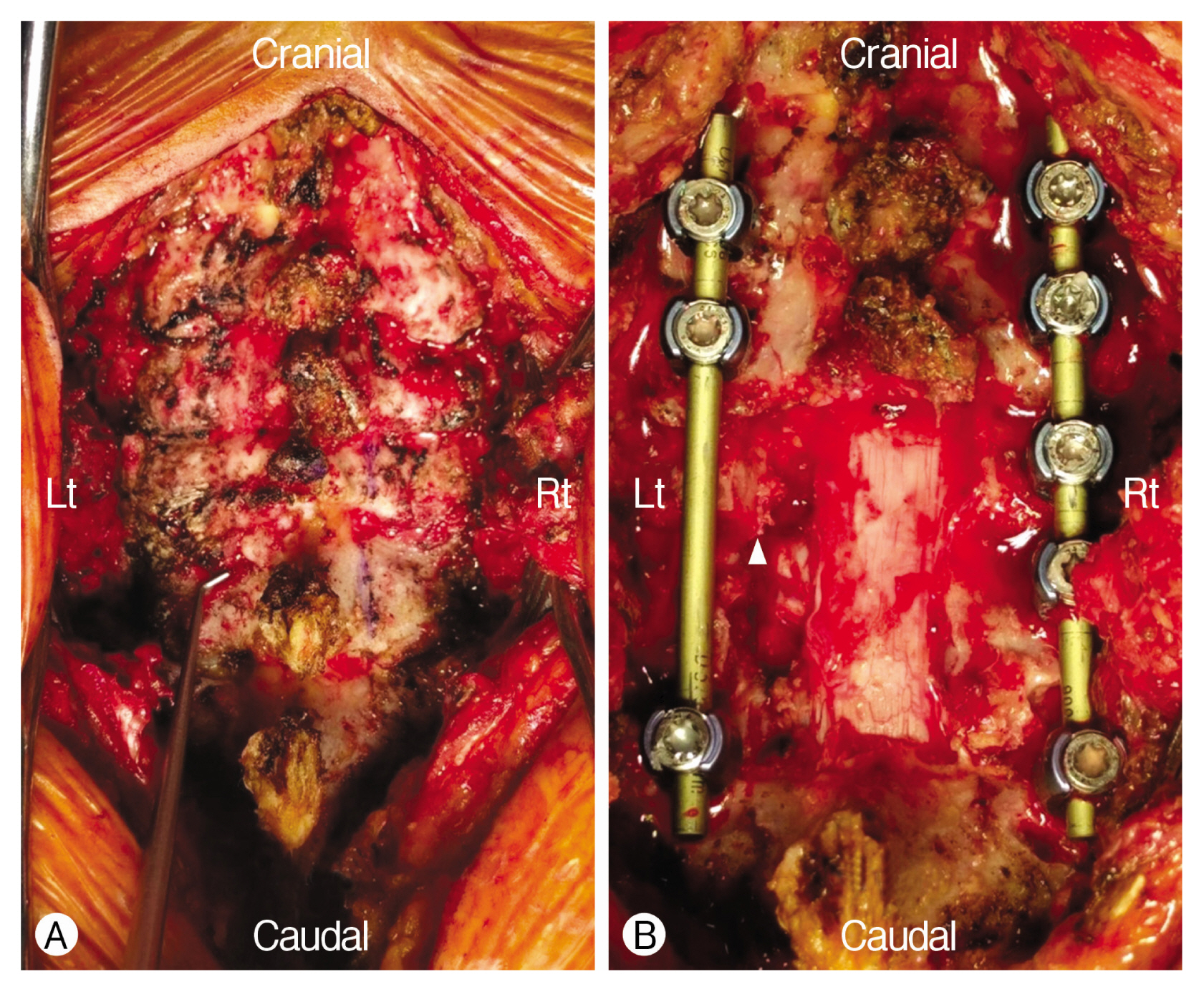
The patient underwent decompression and instrumented arthrodesis of the cervical spine with intraoperative neurophysiological monitoring. En bloc, total laminectomy of C6, 7 was carried out using a high-speed drill for bony decompression. Given a working diagnosis of benign bone tumor based on preoperative imaging findings, laminectomy margins were not extended beyond the area of hyperostosis to avoid vertebral artery injury. After laminectomies, no residual compression of the left C7 nerve root was evident. C4, 5, and 6 lateral mass screws and C7 and T1 pedicle screws were inserted. Screws at C6, 7 were inserted only on the right side because left side insertion points were compromised by wide decompression (Fig. 4)1). Intraoperative monitoring did not show any significant change during the surgical procedure14).
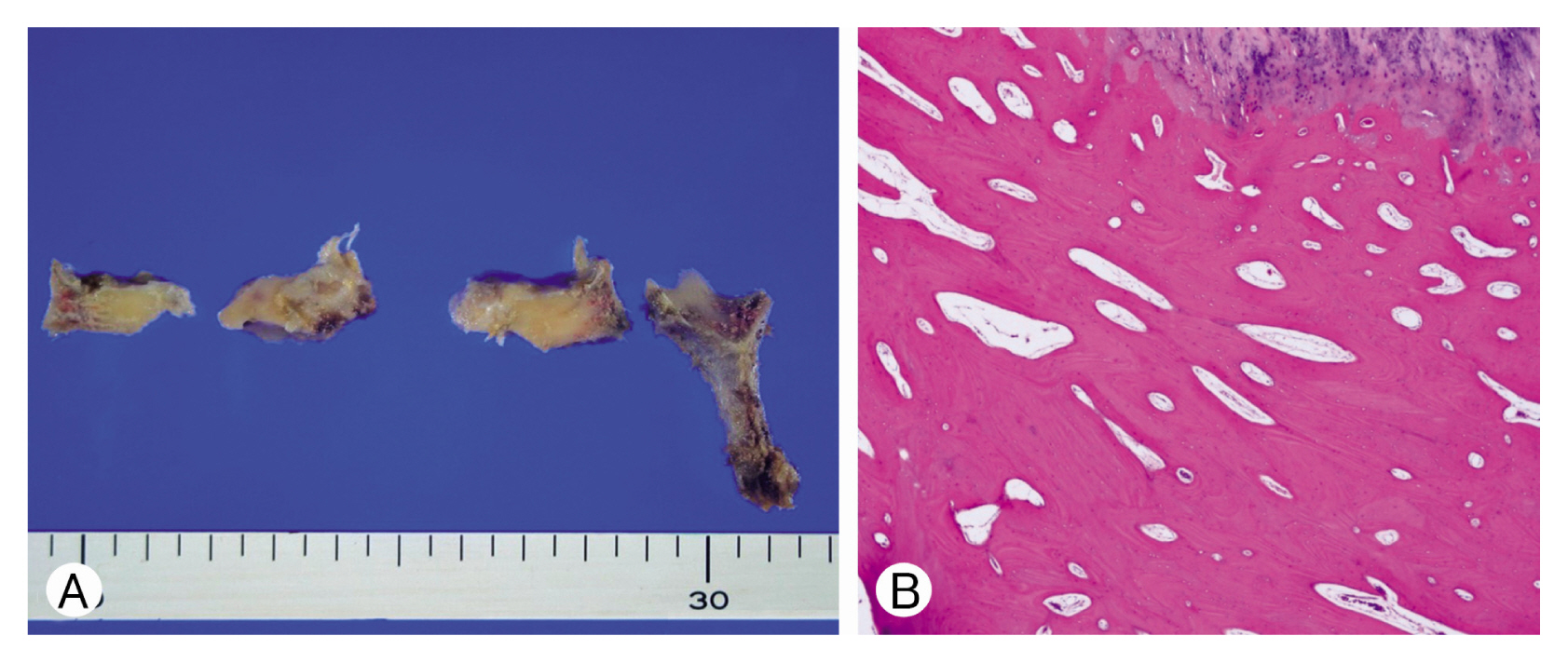
Macroscopically, the internal surface of the lamina was diffusely thickened with a globoid mass protruding from the inner surface. The serial section revealed that the thickened lamina was composed of pearly white or ivory-like compact cortical bone. Representative sections were decalcified and embedded in cassettes, but no definite tumor cells were observed in hematoxylin-eosin stained sections. Whereas lamina trabecular bony tissue remained normal, hyperdense mature cortical bone resulted in cortical and subchondral hyperostosis around the lamina, which was consistent with melorheostosis (Fig. 5).
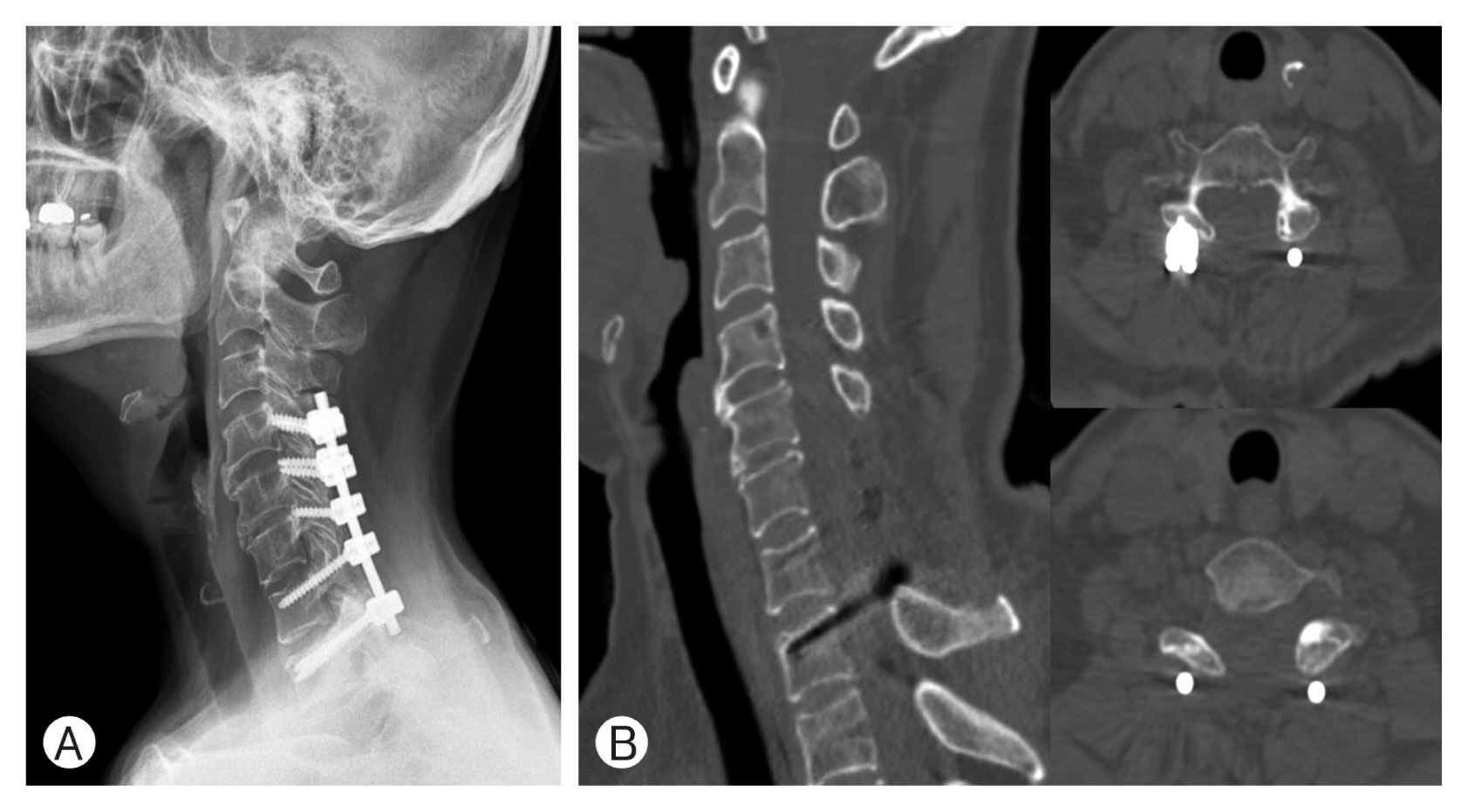
Postoperatively, the patient recovered well without any neurological deficit. Motor function remained intact, and the arm pain improved immediately after surgery. Actually, she only complained of pain around the surgical site. The patient was discharged from the hospital one week after surgery. At a follow-up examination 2 years after surgery, the patient was doing well without recurrent radicular pain (Fig. 6).
DISCUSSION
Melorheostosis is a benign, non-hereditary disease characterized by dense, sporadic sclerosis of skeletal and adjacent soft tissue. The incidence of melorheostosis is 0.9 cases per million18). Spinal involvement of melorheostosis is extremely uncommon because melorheostosis typically affects appendicular bone17). Affected ages vary from childhood to old age and sexes are equally affected. The name of the disease was derived from the Greek word (melos=limb, rhein=flow, ostos= bone formation), which describes the shape of melting wax flowing down a candle. The pathophysiology of melorheostosis remains unclear, although it is presumed to be associated with inflammatory change due to infection, an early fetal developmental anomaly, or ischemic change2).
To the best of our knowledge, only 9 cases of spinal melorheostosis requiring surgical treatment have been issued since the first case report of melorheostosis involving the spinal column was released in 19823). These cases involved 5 males and 4 females aged from 21 to 57 years, though most were diagnosed in their thirties or forties. Sizes and locations of this condition varied widely and do not show any specific pattern (Table 1).
Spinal melorheostosis is generally unilateral and bony expansion is less likely on the opposite side. Vertebral body involvement usually involves the posterior half, though adjacent bones, such as ribs, can also be involved, but not disc spaces 7,10). Recurrences are rare; only one case has been reported5). An open method is preferred for biopsy rather than a percutaneous approach20).
Although the radiographic and bone scintigraphic appearances of melorheostosis have been well described, CT and MRI help confirm and accurately localize zones of hyperostosis in the spine and provide means of assessing degrees of spinal canal and foraminal narrowing8). Although the appearances of soft tissue masses associated with melorheostosis are variable on MR images, mineralized and non-mineralized soft tissue abnormalities should be recognized as they are also manifestations of this disease. MRI aids the diagnosis of melorheostosis and enables the accurate detection and determination of soft tissue involvement and its extent10).
The differential diagnosis of superficial hyperattenuated vertebral and adjacent paraspinal abnormalities includes melorheostosis, tumoral calcinosis, tumoral calcium pyrophosphate dihydrate deposition disease, ivory osteomas, heterotopic ossification (myositis ossificans), and parosteal and periosteal osteosarcoma 11).
Indications for surgical decompression are the same as those for advanced spondylosis, and the aim of surgery is to relieve pressure on affected neural elements21). As shown in Table 1, spinal melorheostosis may be treated by biopsy, decompression, or decompression and instrumented fusion as determined by considerations of patient symptoms and radiologic test results.
Basic follow-up requires periodic plain radiographs to enable the detection of lesion size changes and to check for spinal fusion following surgery. More detailed imaging in the form of CT or MRI may also be required and close clinical follow-up of neurological status is important.
No case of melorheostosis involving the spine has recurred. However, given the limited number of reported cases, it is not possible to determine whether total removal of the affected area should be attempted. In the described case, there was no adhesion with dura, but as melorheostosis is characterized by hyperostosis and hardening of soft tissues, this possibility should be borne in mind during surgery.
CONCLUSION
After reaching a diagnosis of melorheostosis, the patient was treated surgically for radiculopathy without complication. Two years later, a follow-up CT scan disclosed no recurrence of melorheostosis, and clinically the radiculopathy and hypoesthesia had fully improved. Spinal melorheostosis is a rare condition and needs to be differentiated from other bone tumors and vertebral lesions, and thus, biopsy through surgery is sometimes required. Although no case of recurrence has been reported, the possibility must be addressed by continuous follow-up. Importantly, a patient’s symptoms should be carefully considered when deciding whether to observe after biopsy or perform additional decompression.