INTRODUCTION
Traumatic brain injury usually results from a violent blow to the head. Serious traumatic brain injury can result in a skull fracture, epidural hematoma, cerebral contusion, or subdural hematoma(SDH). A SDH is most often the result of trauma. Rarely, there are patients who suffer SDH without a definitive history of head trauma. Nontraumatic or spontaneous SDH is rare and many causes should be considered. The etiology of non-traumatic SDH includes cortical aneurysmal rupture, neoplasm, and spontaneous intracranial hypotension. In this report, we present a case of non-traumatic SDH caused by glioblastoma (GBM).
CASE REPORT
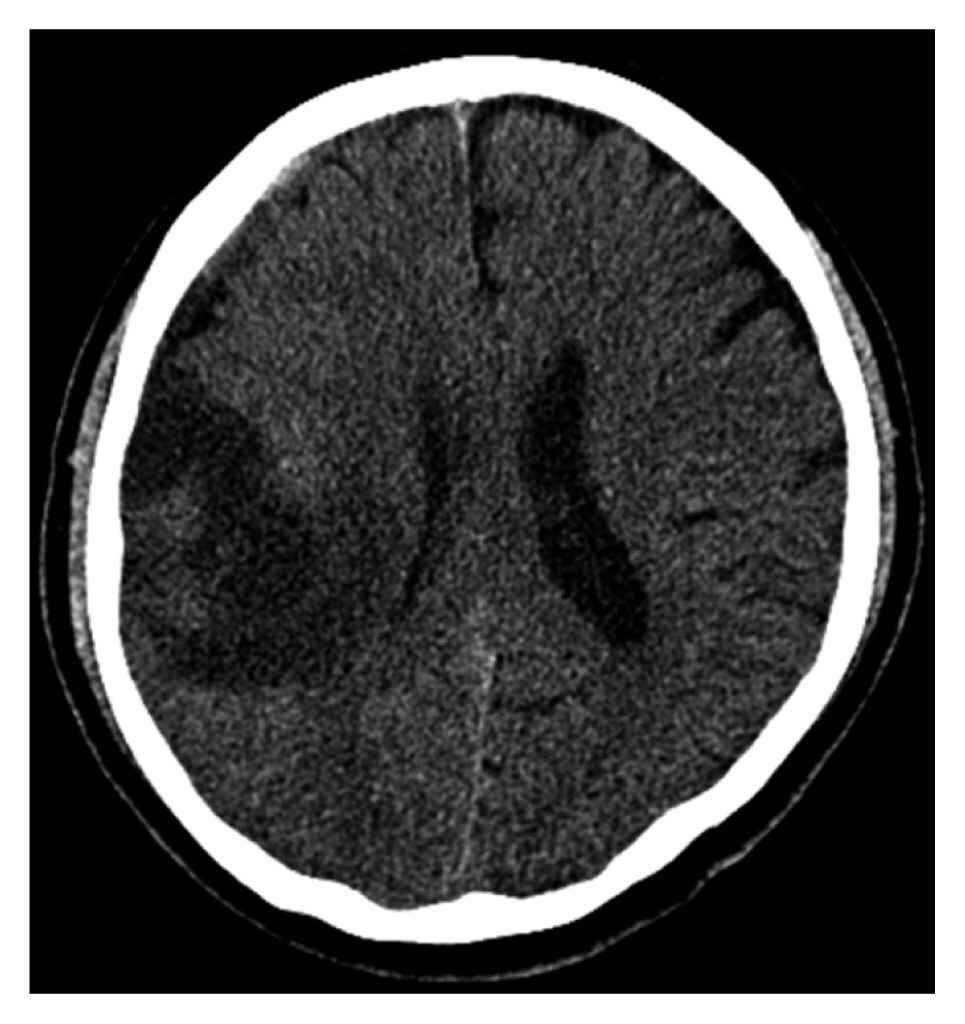
A 76-year-old man presented to another hospital with recurrent left side weakness that had begun several months prior without a history of head trauma. Brain computed tomography (CT) was performed and revealed acute and chronic mixed type SDH on the right convexity (Fig. 1). At that time, the medical team made a decision for the patient to be on conservative care, because the amount of SDH was subtle and the patient’s symptoms were mild.
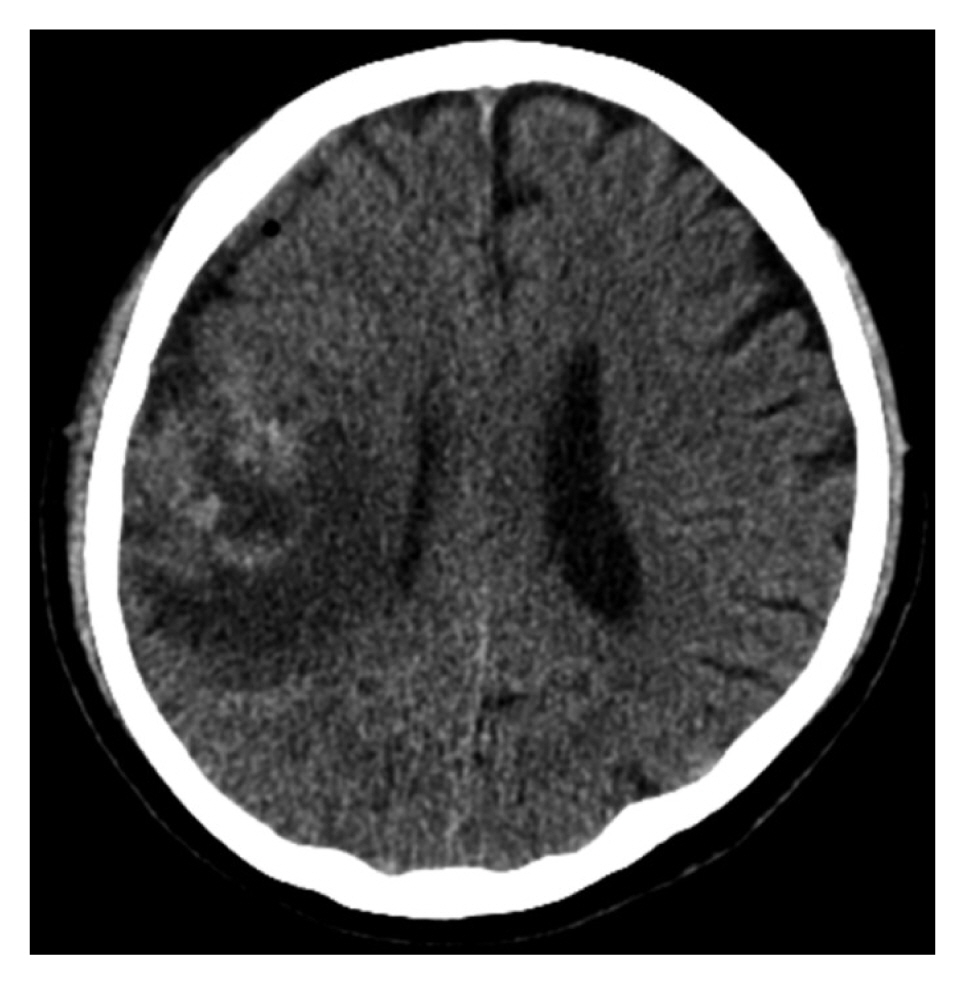
After one month, the patient’s symptoms did not improve and left side weakness and hypoesthesia was aggravated; hence, the patient has transferred our hospital for further workup and management. Brain CT was performed and revealed SDH and new low-density lesion on the right frontoparietal area (Fig. 2). First, we assumed the newly observed lesion was a fluid collection from subdural hygroma or cerebral infarction. We expected the symptoms to be aggravated due to SDH and fluid collection and decided to perform surgical treatment via burr hole trephination for SDH drainage. After surgical management, a dark brownish fluid, a hallmark of typical chronic SDH, was drained. However, the amount of fluid drained was not significant and the patient’s symptoms were not improved.
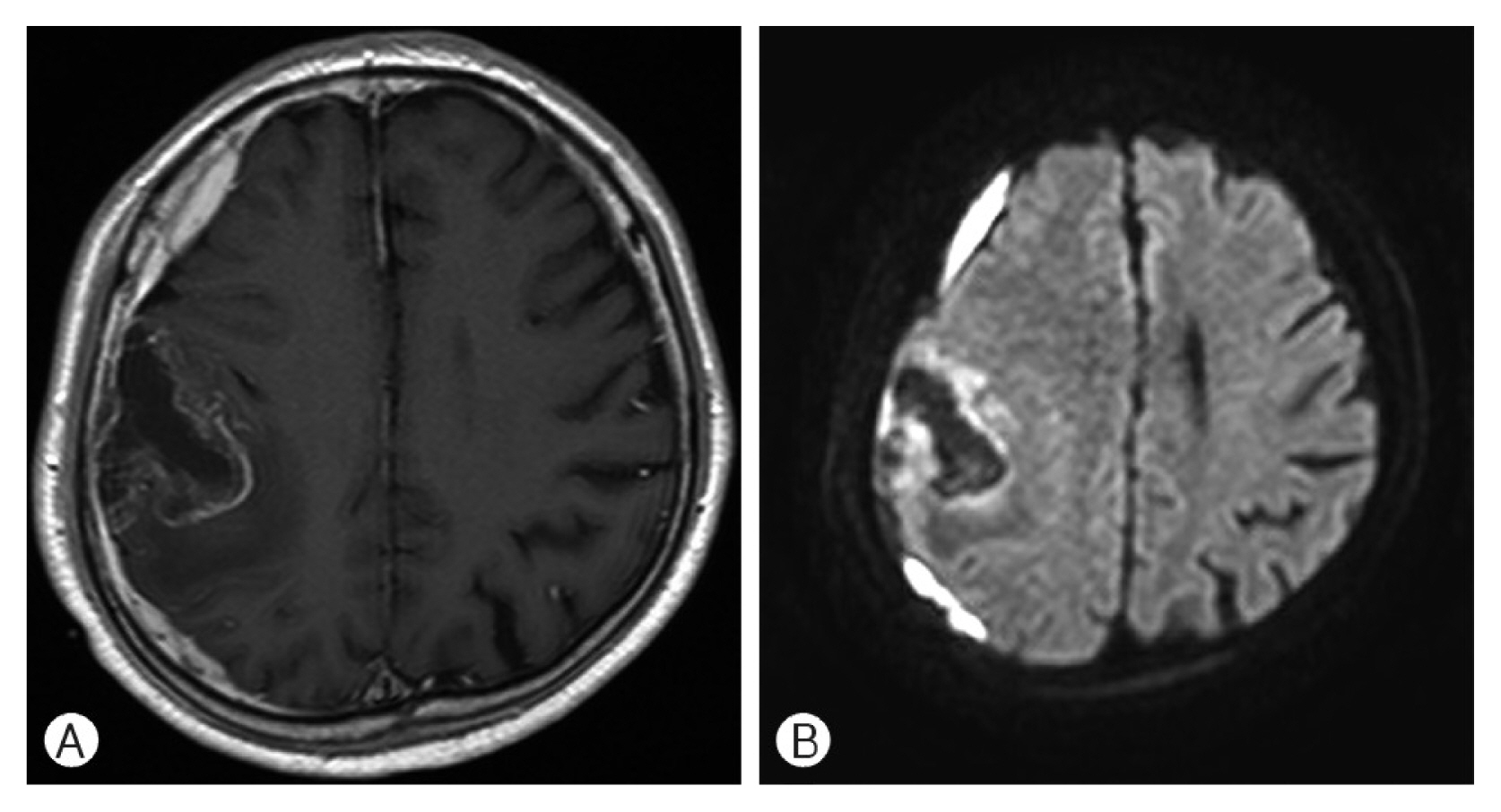
Postoperative brain CT showed a subtle reduction in SDH and a new high-density lesion at the site of the previous low-density lesion (Fig. 3). For evaluation of this new lesion, a full-sequence brain magnetic resonance (MR) imaging (MRI) was performed. Brain MRI revealed a heterogeneous peripheral enhancing irregular mass-like lesion with perilesional edema, for which we could not exclude brain tumor (Fig. 4). Craniotomy was performed for mass-lesion biopsy and removal. The result of mass-lesion biopsy was GBM.
The results of biopsy was GBM
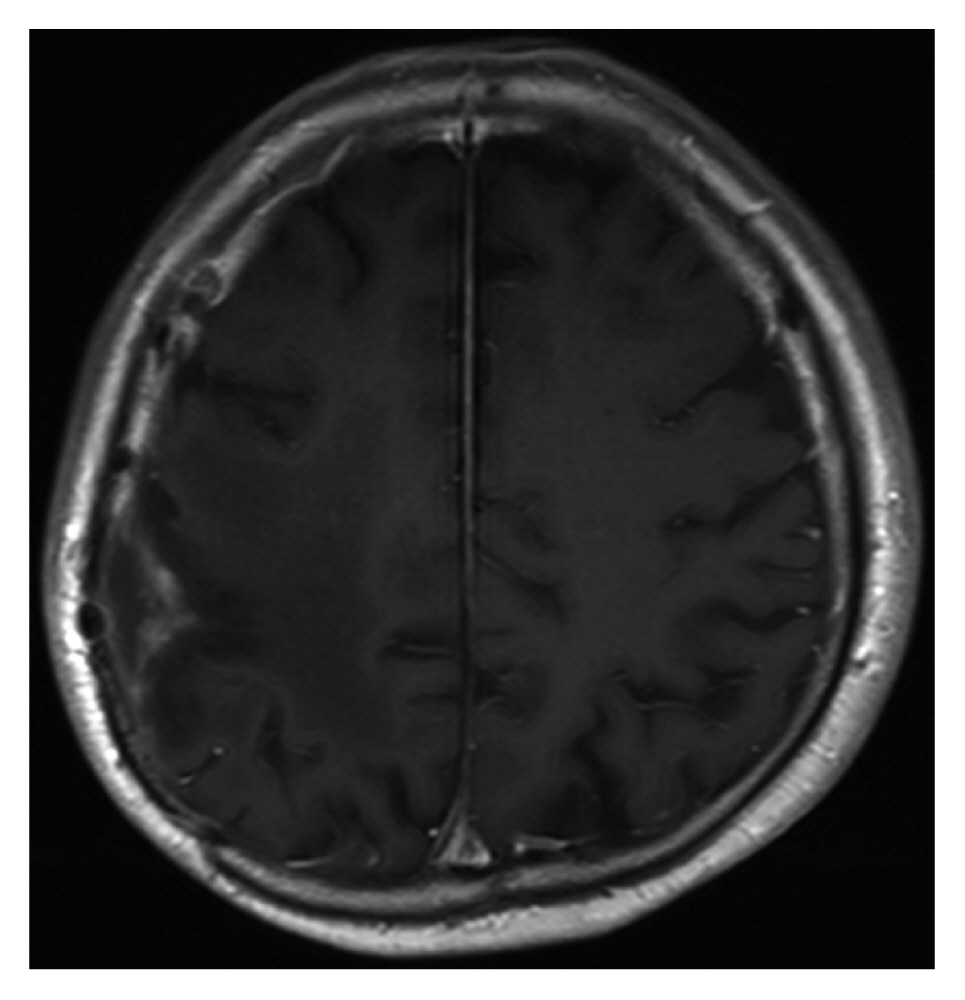
Follow-up brain MRI examination showed the lesion was almost totally removed(Fig. 5). The subsequent concordant radiochemotherapy, which was initiated four weeks after surgery, was tolerated very well.
DISCUSSION
In general, patients with SDH have a history of head trauma. However, some SDHs without trauma history is observed. A broad cause of spontaneous SDH should be considered including vascular and even neoplastic origin. Coombs et al.5) reported that among the 63% of cases where patient sex was specified, there was a 2:1 male predominance; overall, the majority of causes of spontaneous SDH were arterial (61.5%), then idiopathic (10.8%), coagulopathic (10.1%), neoplastic (5.4%), and spontaneous intracranial hypotension (5.4%).
The known vascular origins of non-traumatic SDH are ruptures of small cortical arteries or intracranial aneurysms, rupture of arteriovenous malformation (AVM), and hypertensive or amyloid angiopathic intracerebral hematoma (ICH) perforating the brain surface and arachnoid membrane1,3,5,6,20,22). Aneurysmal rupture usually produces subarachnoid hemorrhage (SAH) with or without ICH and/or intraventricular hematoma (IVH). Aneurysmal SDH with or without SAH is rare, with an incidence estimated to be between 0.5% and 7.9%20). A rare case of non-traumatic acute SDH without SAH, which was caused by rupture of a cortical artery aneurysm, was reported and the patient did not have an infection, inflammation, neoplasm, or head trauma1). The pathogenesis of distal MCA or cortical artery aneurysms includes infectious or neoplastic emboli, arteritis, head trauma, and arterial dissection21). In cases of AVM rupture, ICH is the most common, followed by IVH and SAH. Some authors reported rare cases of SDH due to rupture of cortical AVM and thought AVM vessel adhesion to the arachnoid membrane and strain on the arachnoid membrane could have led to the formation of SDH rather than SAH or ICH3,6). Rupture of a leptomeningeal artery adjacent to the dura, with extravasation into both the brain parenchyma and the subdural space, is a possible explanation of SDH and non-traumatic primary lobar ICH22).
Spontaneous ICH is the most common bleeding complication in a patient with coagulopathy or on antiplatelet or anticoagulant therapy, followed by non-traumatic SDH or infrequent SAH2,7). Although the pathogenesis of non-traumatic SDH with coagulopathy or anticoagulant therapy remains unclear, many studies reported that the mortality rate in patients with acute or chronic SDH and coagulopathy was higher7,13).
Spontaneous intracranial hypotension (SIH) is another well-known cause of non-traumatic SDH. SIH is sometimes associated with bilateral chronic SDH. The incidence of SDH among SIH patients ranges from 16% to 57%, predominantly in males, whereas SIH without SDH predominantly occurs in females8,14,18,30). Low cerebrospinal fluid pressure generates tears in the bridging veins of the dural border cell layer, followed by vein rupture5,25).
Intracranial tumors are a well-known cause of hemorrhage into the brain parenchyma. Clinical and autopsy studies have reported that brain tumors were found in 0.9% to 11% of spontaneous ICH19,26,29). However, non-traumatic SDH associated with neoplasm is believed to occur rarely and has several pathogenesis including hemorrhagic effusion from malignant tissue, dural vessel obstruction by neoplastic cells, angio-demoplastic reaction of the dura to tumor infiltration, and direct hematogenous metastasis of malignant tumor17,23,26,29). The incidence of brain hemorrhage from metastatic and primary intracranial malignant tumors is similar. Lung cancer9), melanoma19), and renal cell cancer28), as well as choriocarcinoma24), are implicated most frequently when brain hemorrhage results from a metastatic lesion. Oligodendroglioma or GBM primary intracranial tumors are often reported to be associated with hemorrhage4,10,11, 15,16,27). One retrospective study reported that the hemorrhage rate for mixed oligodendroglioma/astrocytoma was higher than GBM12).
Most SDHs are generally thought to be caused by head trauma and can happen in any age group. Brain CT scans are usually sufficient for diagnosis in cases of traumatic SDH. When a SDH patient presents without a history of head trauma, the differential diagnosis should include various causes, as mentioned above, and be evaluated via neuroimaging modalities including brain MRI and CT, and/or MR angiography in addition to complete medical history.
CONCLUSION
SDH is typically a sequela of head trauma; however, some cases without a definitive history of head trauma. So-called non-traumatic or spontaneous SDH can occur due to various causes like vascular lesions, neoplasms, coagulopathies, and SIH. When a patient suffers from SDH without a clear history of head trauma, it is wise to conduct additional examinations, such as CT angiography or brain MRI, to help determine the cause of SDH and to plan further treatment.