INTRODUCTION
With recent advances in treatment technology, the mortality rate from spinal abscesses is decreasing. However, spinal abscesses are still unusual and difficult to treat3). In general, spinal abscess occurs frequently in the epidural space, but rarely invade as intradural lesions2,7). According to the Massachusetts General Hospital between 1947 and 1974, the annual incidence of spinal epidural abscesses has risen in the past 2 to 3 decades from 0.2 to 1 case per 10,000 hospital admissions to 2.5 to 5.1 per 10,000 admissions7). This study reports the management of a 56-year-old woman with epidural and subarachnoid spinal abscesses due to acute pyelonephritis.
CASE REPORT
A 56-years-old woman with a medical history of acute hepatitis and osteoarthritis entered the hospital. She did not have diabetes mellitus, and there was no prior spinal intervention history. Her symptoms were lower back pain and pain in both flanks that started one day before the visit, and fever and chills that started two days before the visit. Initially, she showed lower limb extremity motor weakness as bilateral hip grade III/V, bilateral knee grade III/V, and bilateral big toe/ankle grade IV on the neurologic exam. On the admission date, she had a fever of 38°C and chills. On hospital day 1, costovertebral angle tenderness appeared in both flanks and the pain was more severe on the left than on the right side. An abdominal-pelvic computed tomography scan was performed. The results showed right focal acute pyelonephritis of the upper portion of the kidney. The blood inflammation markers were increased, showing an erythrocyte sedimentation rate (ESR) of 85mm/hr (0-10mm/hr), a C-reactive protein (CRP) level of 29.11mg/dL (0-1 mg/dL). Klebsiella pneumoniae was cultivated in the blood and urine cultures. In the department of internal medicine, the antibiotic meropenem was administered.
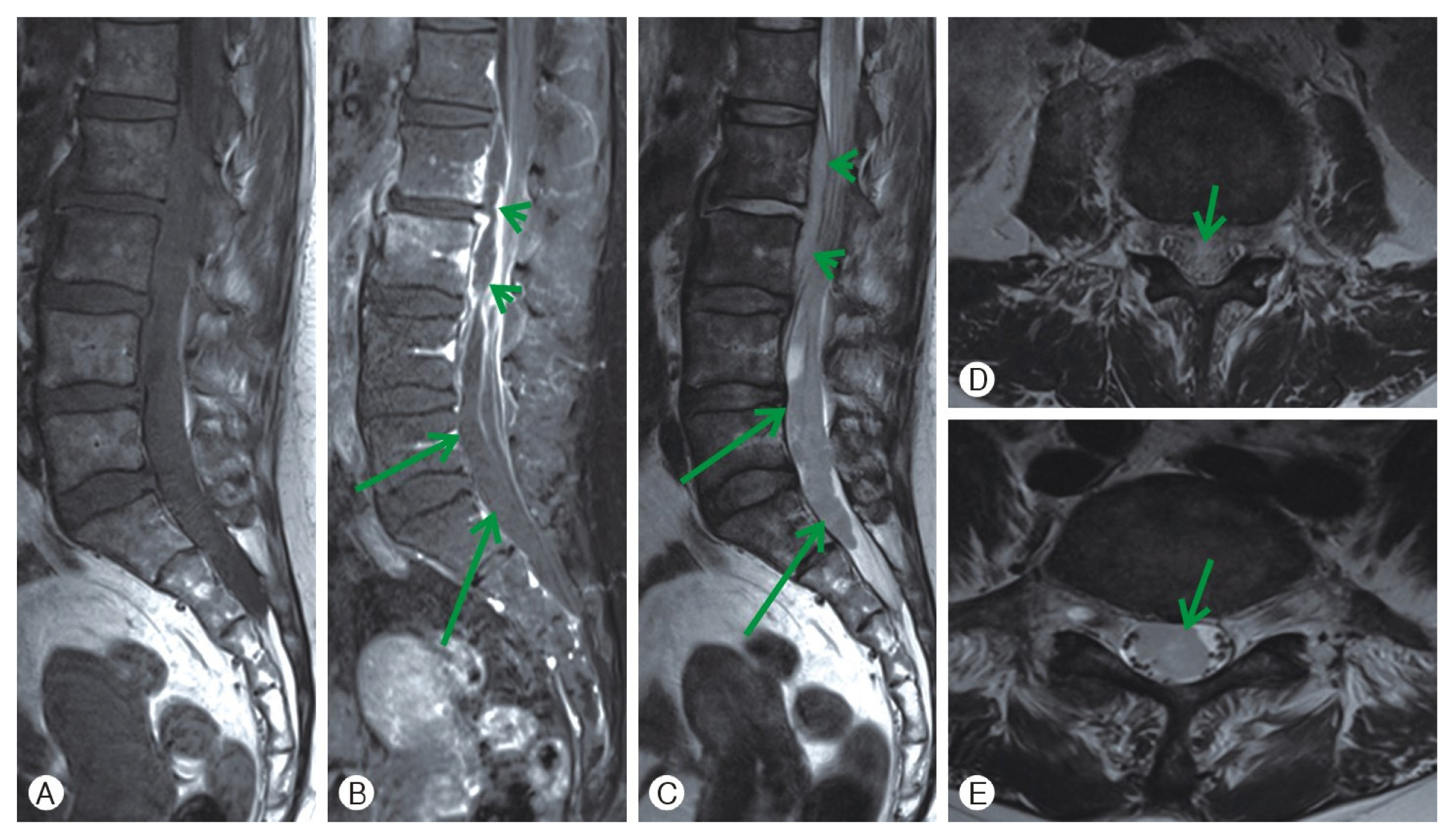
Spine magnetic resonance imaging (MRI) was performed and the results showed an epidural abscess at the L2-3 level causing central canal compromise and a ventral dural tear at the L3 lower vertebral endplate level with an intradural extension of the abscess at the L3-S1 level and combined arachnoiditis (Fig. 1).
Surgical intervention was needed because of the lower limb extremity motor weakness and the subdural empyema progression in spite of medical treatment. With the patient under general anesthesia, the surgery was performed with the patient in the prone position on the Jackson table. After confirming the surgical site on the radiograph, a dorsal midline incision was made. Total laminectomy at L2-3 and laminotomy at L4-5 were performed to removal the spinal abscess. At the L3 vertebral body lower margin level, a central ventral dura defect sized at 0.5×0.5-cm and cerebrospinal fluid leakage were confirmed. Bilateral L3 dorsal roots swelling was seen. After irrigation, wrapping was performed around the dural defect using artificial dura. The surgery was completed uneventfully and the patient was taken to the Intensive Care Unit.
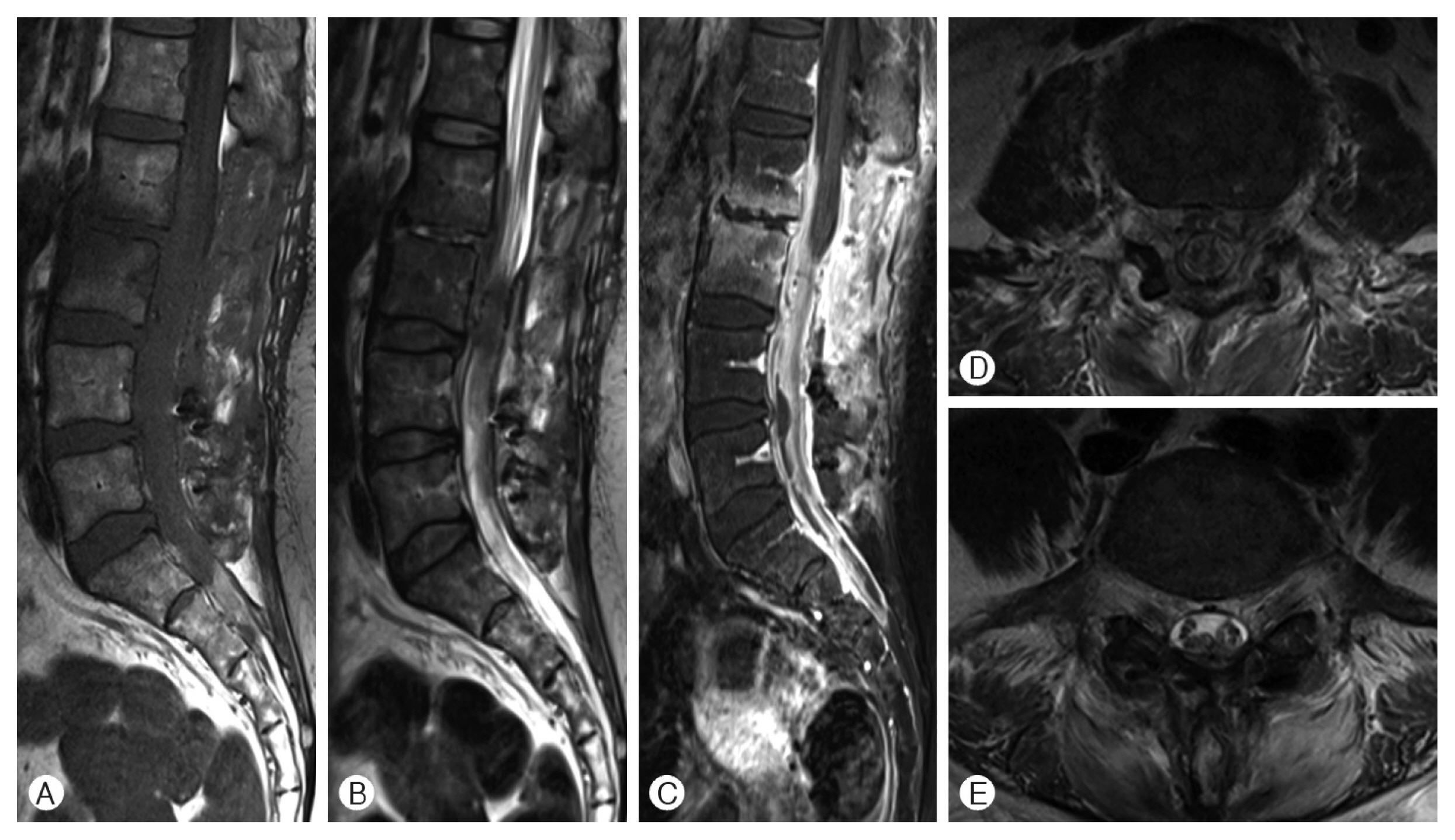
After surgery, back pain subsided enough. However, lower limb extremity motor weakness was not recovered. It was perhaps considered as the effect of dorsal roots swelling during removal of the spinal abscess. No growth was seen in the pus culture performed in the operation room, so antibiotics treatment was started as an unknown origin cerebral nervous system(CNS) infection. Ceftriaxone, vancomycin and metronidazole antibiotics were administered for the patient’s CNS infection. No growth was seen in the follow-up blood culture. She exercised for seven weeks and was able to walk at the time of discharge. Three months after admission, a postoperative lumbar spine MRI with contrast enhancement was performed (Fig. 2). The MRI shows decreased prevertebral phlegmons and epidural abscesses at the L2-3 level with resolved central canal compromise and postoperative changes combined with remaining phlegmons in the epidural space and arachnoiditis at L4-5. At the last follow-up, the inflammatory markers decreased to ESR 21mm/hr, and CRP 0.1mg/dL. From admission to discharge, meropenem, vancomycin, and metronidazole were administered for more than one week, and ceftriaxone was administered for nine weeks.
DISCUSSION
Spinal epidural abscesses are rare, but an epidural abscess accompanied by an intradural abscess is much rarer2,7). Mortality increases if the infection is not controlled by antibiotics or progresses further to become meningitis. Therefore, accurate diagnosis and treatment are very important. A spinal abscess is an infection, so using long-term antibiotics after abscess removal surgery is very important. Also, an extensive treatment course is needed to rehabilitate the patient.
Of the spinal abscess patients, 70% are men, and 68% of the women are 31 to 70 years old7). The incidence in men was reported to be twice that in women7). The primary spinal abscess pathogen is Staphylococcus aureus in 70% of the cases and Streptococcus in 7%1,2,7). In our case, there was no growth in the abscess culture, but the blood and urine cultures indicated Klebsiella pneumoniae. This was a very unique case because it was different from the common reports of spinal abscesses.
Factors like diabetes mellitus, end-stage renal disease, septicemia, human immunodeficiency virus infection, malignancy, steroid use, intravenous drug abuse, alcoholism, distant site infection, and an indwelling catheter can cause a spinal abscess2,6,7). In our case, the patient had acute pyelonephritis, and the MRI showed osteomyelitis and prevertebral phlegmons on L2 and L3. The MRI showed a ventral dural tear at L3 of the lower vertebral endplate level, suggesting that the formation of the intradural abscess was through a dural tear.
Spinal abscesses are initially treated with antibiotics for a period of time. However, when neurological symptoms develop, decompressive surgical abscess removal is required5). Depending on the observed clinical and laboratory responses, such as ESR or CRP levels, some authors advocate only intravenous therapy for 6 to 8 weeks, while others suggest parenteral therapy for 6 to 8 weeks and oral therapy for more than 2 consecutive months4). After successful surgery, we used antibiotics to target Klebsiella pneumoniae for 10 to 11 weeks and the patient was in a rehabilitation program. After rehabilitation, she was able to walk by herself. Although spinal abscesses are associated with high mortality, the patient was discharged after a rehabilitation program, indicating a good outcome.
This report described an epidural and subarachnoid abscess in a middle-aged woman due to acute pyelonephritis caused by Klebsiella pneumoniae. With surgery and antibiotic treatment, the patient’s symptoms improved significantly without any complications. And the motor weakness that occurred after surgery was greatly improved with active rehabilitation.