INTRODUCTION
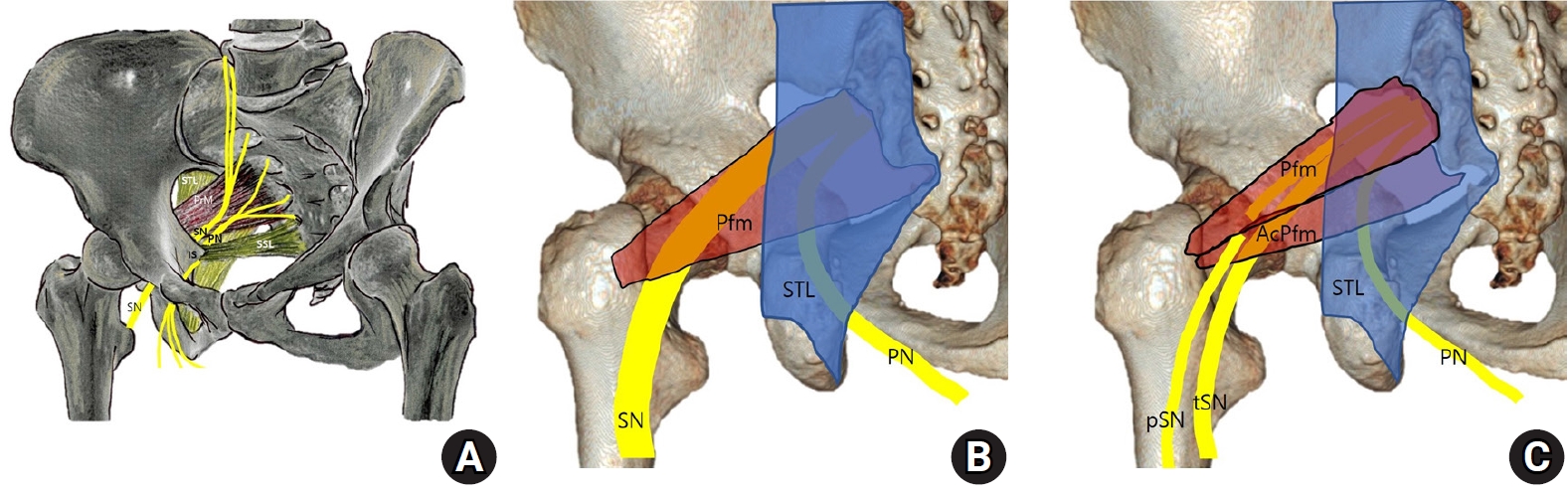
Entrapment of the sciatic nerve at any point along its course can result in a clinical syndrome of buttocks and leg pain known as sciatica, with a reported incidence as high as 43%13,15). A less common and under-diagnosed cause of sciatica is sciatic nerve entrapment in the gluteal region (formerly called pyriformis syndrome)9). Piriformis syndrome was classically thought to result from hypertrophy and inflammation of the pyriformis muscle involving an estimated 6% to 8% of all sciatica cases13). Anatomical variations of the piriformis muscle are important among multiple causes of sciatic nerve entrapment involving the subgluteal space13). Six anatomical relationships between the sciatic nerve and piriformis muscle (Fig. 1) were first described by Beaton and Anson in 19374,20). Sciatic entrapment can occur in both type 1 and type 2 variations of the sciatic nerve in the subgluteal space21). Patients with sciatic nerve entrapment who do not respond to conservative treatment generally require surgical decompression9,21).
The transgluteal approach allows access to lesions involving the hip, the sciatic nerve, and the pudendal nerve via dissection of the gluteus maximus muscle in the buttock. Sciatic nerve entrapment, previously known as piriformis syndrome9), has recently been classified as a deep gluteal syndrome (DGS)7). The incidence of hip and leg pain due to sciatic nerve entrapment remains unknown. However, its importance has recently been emphasized as one of the causes of failed back surgery syndrome and DGS7,9).
In our experience, several problems were encountered when planning decompression surgery for sciatic nerve entrapment. First, the transgluteal approach through dissection of the gluteal muscle was unfamiliar to neurosurgeons. Second, the transgluteal approach for orthopedic hip surgery was basically a posterolateral approach to the hip joint rather than direct access to the sciatic nerve. Third, direct surgical approach to the sciatic nerve was not covered in detail even in a recent comprehensive textbook of peripheral nerve surgery5). Therefore, when planning sciatic nerve surgery, it is difficult to find references on the extent of decompression, method, and structures. Therefore, we applied a transgluteal approach for entrapment of the pudendal nerve located immediately adjacent to the sciatic nerve to address the sciatic nerve and the piriformis muscle and tendon running under the sacrotuberous ligament (STL)3,14,21). The objective of this report was to introduce a specific method of transgluteal approach for sciatic nerve decompression based on our experience of 30 cases over the past four years.
MATERIALS AND METHODS
1. Localization and Incision for Transgluteal Approach
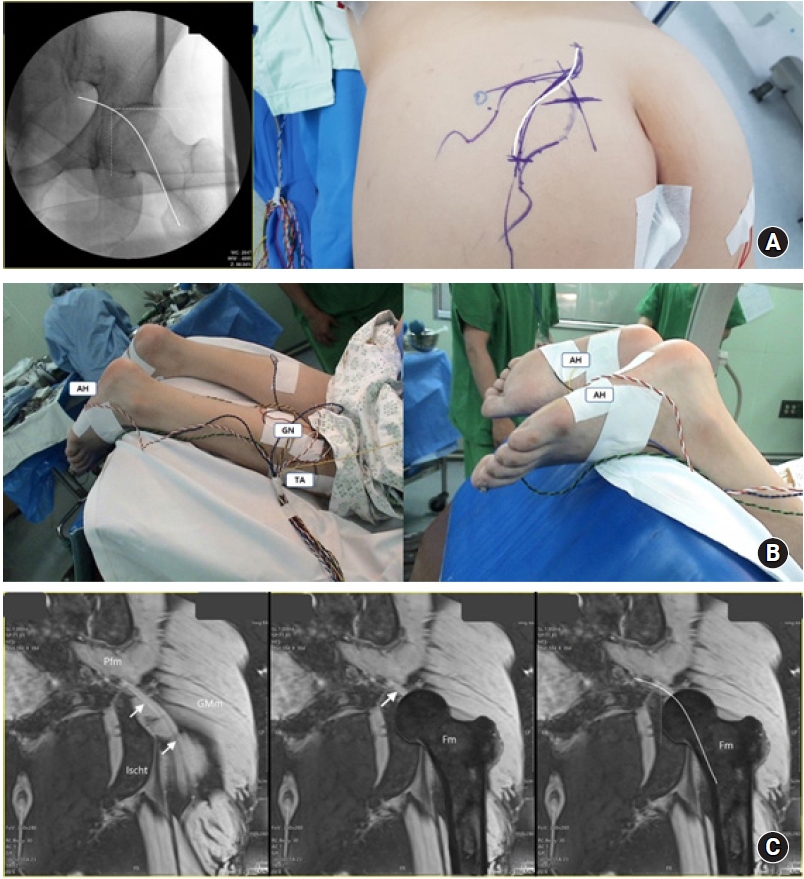
Under general anesthesia, the patient was placed in a prone position on a radiolucent frame where the position of the femoral neck could be confirmed (Fig. 2A). Intraoperative neurophysiological monitoring was routinely performed to identify tibial and peroneal (fibular) divisions of the sciatic nerve, inferior gluteal, and posterior femoral cutaneous nerves during surgery and to prevent nerve damage. For intraoperative nerve stimulation and mapping, recording electrodes were placed in the abductor hallucis and gastrocnemius muscles innervated by the tibial nerve and the tibialis anterior muscle innervated by the peroneal nerve (Fig. 2B). When pudendal nerve surgery was performed together, an external anal sphincter was monitored to check the inferior rectal branch of the pudendal nerve.
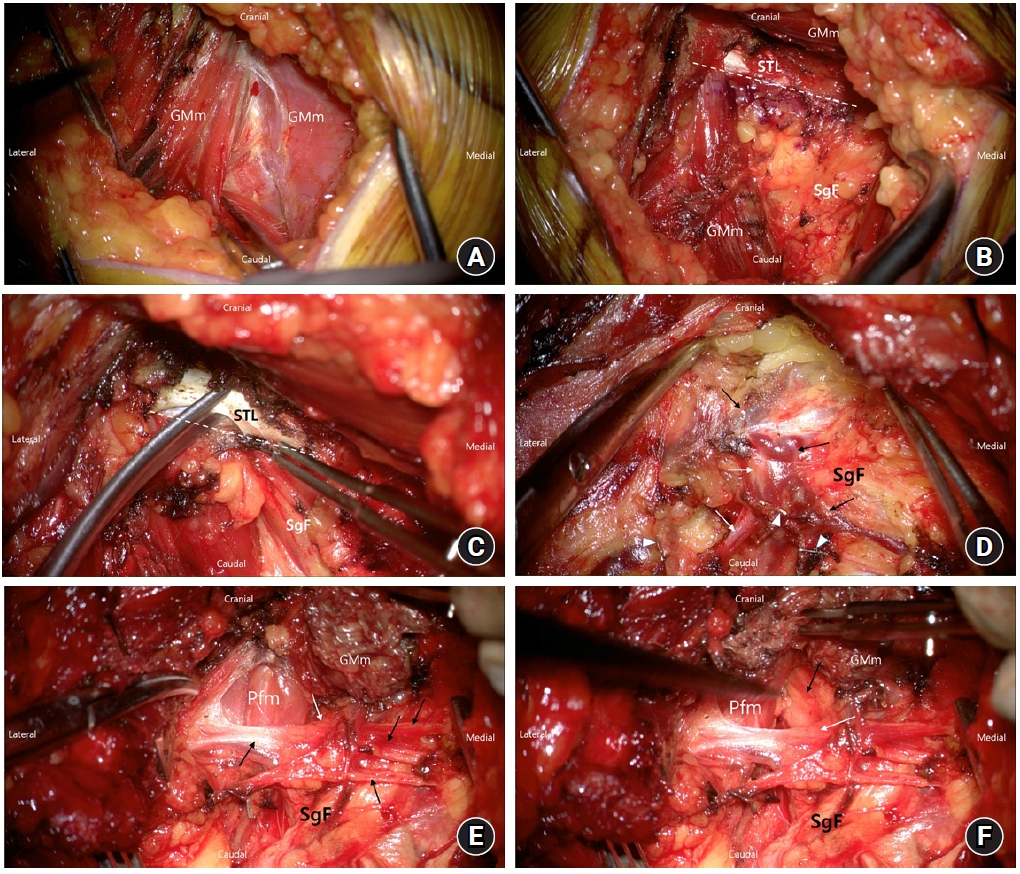
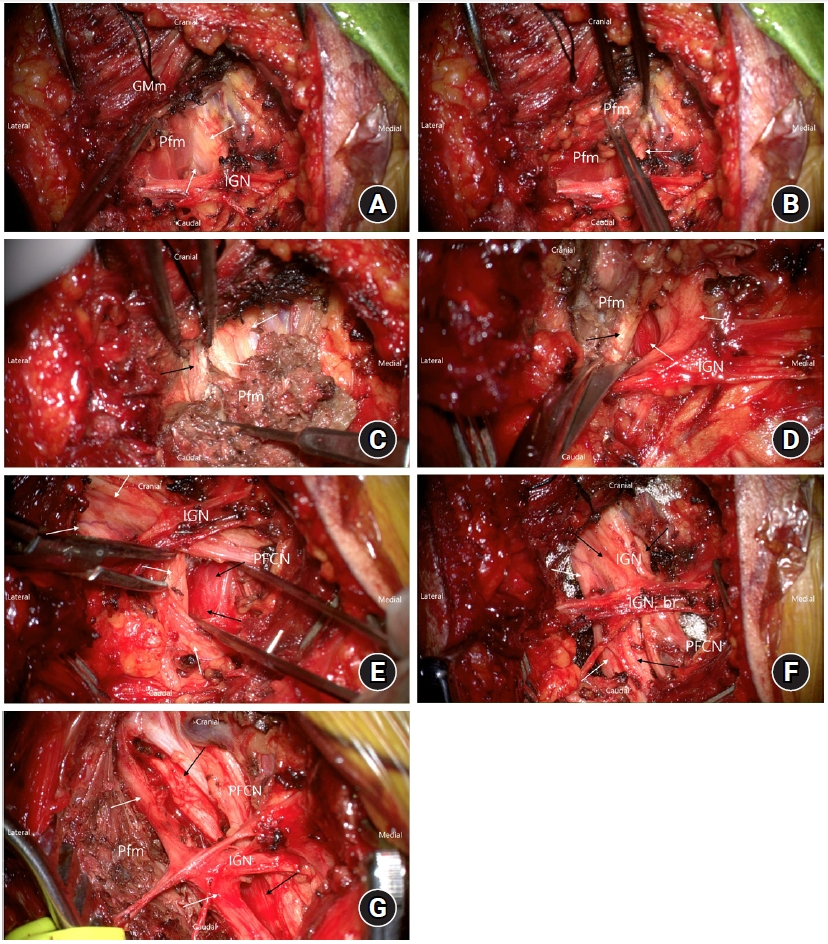
A skin incision was made to allow direct posterior access to the sciatic nerve and its division. The relative path of the sciatic nerve to the neck of the femur was estimated in advance through serial coronal images of the magnetic resonance imaging (MRI) of the pelvis (Fig. 2C). The site of sciatic nerve decompression assessed by MRI ran mostly from the upper medial side of the femoral head through the center of the femoral head to the level of the lesser trochanter on the medial side of the femur (Fig. 2C). The position of the femoral head and neck was confirmed through C-arm fluoroscopy at the neutral position of the affected hip joint and a lazy S-shaped incision with a size of about 8 to 10 cm was marked (Fig. 2A). After dissecting the subcutaneous fat and gluteal fascia, the gluteal muscle, which proceeded obliquely from the medial superior to the lateral inferior, was exposed. The gluteus maximus muscle was dissected along with the muscle texture. It did not need to be cut (Fig. 3A). When dissecting the exposed gluteus maximus, the lateral edge of STL was exposed from above (Fig. 3B). The STL originated from the ischial tuberosity and supported the back of the piriformis muscle encircling the sciatic nerve. Therefore, partial resection of the lateral edge of the STL is recommended for circumferential and anatomically complete decompression of the sciatic nerve. Retraction of the gluteus maximus muscle exposed the STL and subgluteal fat layer (Fig. 3C).
2. Dissection in the Subgluteal Fat Layer
The subgluteal fat layer contains the inferior glueteal nerve and vessels. It is located just above the sciatic nerve, its divisions, and the piriformis muscle. Therefore, it serves as a gateway to the target structure. Dissection of subgluteal adipose layer can sometimes be difficult as it involves the inferior gluteal neurovascular structure. Occasionally, dilated engorged venous structures can interfere with the surgical field of view (Fig. 3D). The inferior gluteal vessels should be separated from the inferior gluteal nerve strands and cut by ligation with hemoclips. The inferior gluteal nerves should be separated from the vessels and preserved. When the dissected fat layer is retracted, the piriformis muscle and sciatic nerve are exposed below (Fig. 3E, F).
3. Exposure of the Sciatic Nerve and Intraoperative Neurophysiology
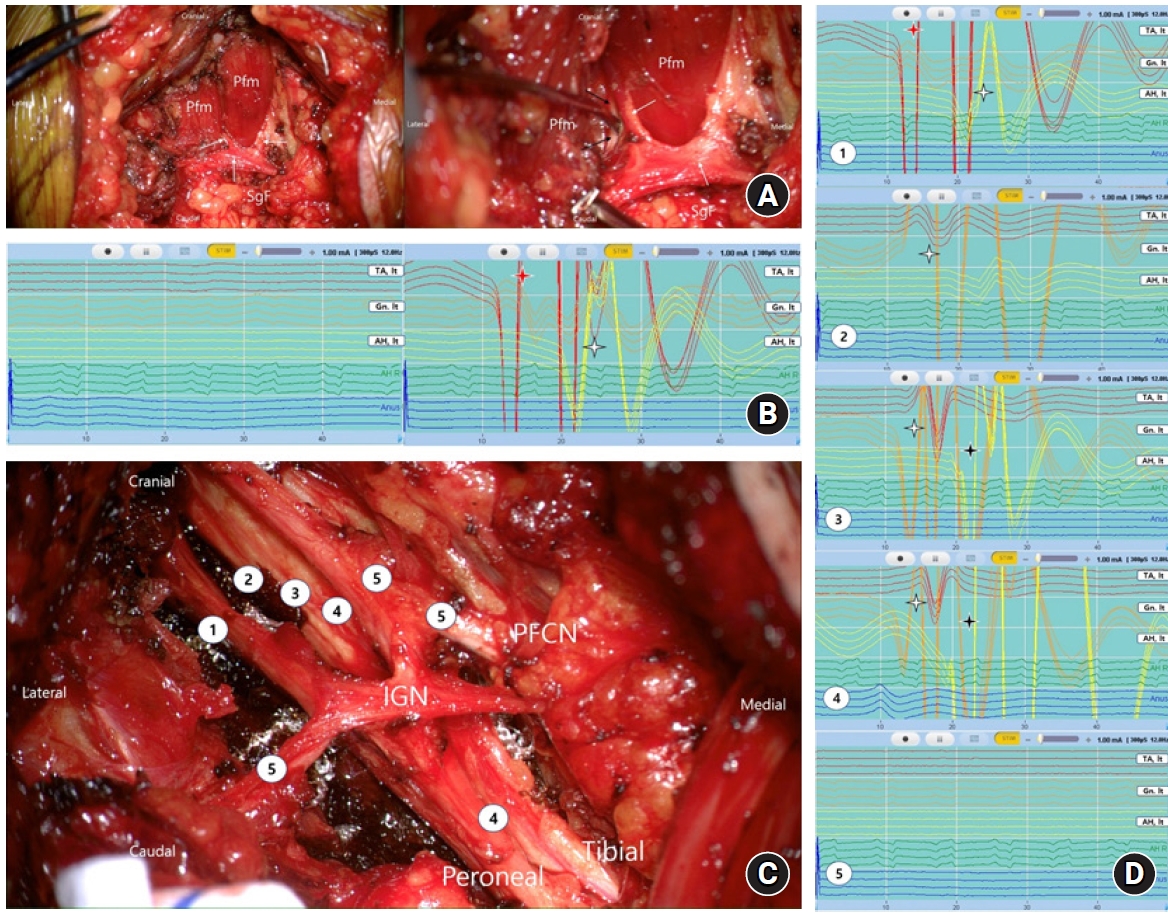
When a portion of the sciatic nerve is exposed, it is important to determine whether it is the tibial division or the peroneal division. In this case, intraoperative nerve stimulation is helpful. Using monopolar stimulation (1 mA, 300 μsec, 12 Hz), an electromyographic (EMG) response was evoked in the sampled leg and foot muscles (Fig. 2). EMG responses of the abductor hallucis and gastrocnemius muscles allowed identification of the tibial division of the sciatic nerve. The peroneal division was confirmed by the EMG response in the tibialis anterior muscle (Fig. 4). Alternatively, stimulation-induced movement of the ankle and foot could be identified. Dorsiflexion of the foot refers to stimulation of the peroneal division. Plantar flexion refers to stimulation of the tibial division. Stimulation of the inferior gluteal nerve and posterior femoral cutaneous nerve did not induce an EMG response in the abductor hallucis or tibialis muscles but caused contraction of the gluteus maximus muscle in the surgical field (Fig. 4A, D).
The reason why it is important to check the peroneal division of the sciatic nerve is that there might be other divisions that have not been discovered yet besides the currently exposed division (Fig. 4A, B). This is especially important in decompression of the type 2 variation, in which the sciatic nerve splits into two parts and runs above and below the piriformis muscle and tendon.
4. Circumferential Decompression of the Sciatic Nerve
After both the sciatic nerve and divisions were identified, the entrapping piriformis muscle was carefully separated from the nerve (Fig. 5A). Holding the piriformis muscle with forceps, coagulation, and cutting the piriformis muscle were performed while preventing thermal damage to the nerve (Fig. 5B). The piriformis muscle was resected from the proximal portion of the piriformis muscle located below the STL (Fig. 5C). It is recommended to cut the piriformis muscle gradually while performing bipolar coagulation to facilitate hemostasis (Fig. 5B, C). Also, when excising the muscle, the piriformis tendon located below the muscle belly should also be excised (Fig. 5C). If the hypertrophy of the piriformis muscle is severe, an additional incision of the STL overlying the piriformis is necessary.
The proximal course of the sciatic nerve located below the compressing piriformis muscle and tendon should be identified by elevating the stump of the resected piriformis muscle and tendon at the proximal level (Fig. 5D). It is not necessary to excise all piriformis muscles located around the sciatic nerve. Only the portion that is attached to and encircling the nerve is removed (Fig. 5C, D). Elevation and retraction of the cut end of the resected piriformis muscle will separate it from the underlying sciatic nerve division. The distal tendon of the piriformis muscle running to the greater trochanter was then excised and removed from the lower portion of the muscle stump (Fig. 5D). When the adherent and encircling portion of the piriformis muscle to the sciatic nerve is removed, the sciatic notch and obturator internus muscle located below the sciatic nerve should be dissected confirm free passage of the sciatic nerve (Fig. 5E). It should be borne in mind that the purpose of surgery is not to remove the piriformis muscle, but to circumferentially decompress the sciatic nerve (Fig. 5F, G).
For type 2 sciatic nerve variation, the small bipartite piriformis muscle and tendon sandwiched between the tibial and peroneal divisions should be removed together (Fig. 4A). Once the laterally located peroneal division is identified and pulled by the vessel loop, the underlying piriformis muscle belly and tendon are carefully separated from the underlying tibial division. When removing the small bipartite piriformis muscle with bipolar coagulation, its tendinous portion should be removed while avoiding heat injury to the nerve (Fig. 5D). When the sciatic nerve and its divisions are decompressed, the underlying ischial spine and the obturator internus muscle are identified. An external neurolysis of the sciatic nerve to these structures is then performed (Fig. 5E). Circumferential decompression of the sciatic nerve should be ensured from its proximal course below the STL to the lesser trochanteric level. Most sciatic nerve entrapment other than ischial tunnel syndrome occurred in the area where the sciatic nerve is attached to the piriformis muscle and its tendons. Free passage of the sciatic nerve from the greater sciatic foramen should be verified. After securing hemostasis, an anti-adhesion gel or film was placed around the nerve to prevent nerve adhesion. Leaving a 100 mL drain in the subgluteal space, the overlying wound was closed in layers. Pain following surgery was moderate. Most patients could sit and walk from the next day.
DISCUSSION
1. Differences between Several Transgluteal Approaches for the Sciatic Nerve
The authors presented a transgluteal approach specialized for circumferential decompression of the sciatic nerve pathway. In the sense of splitting the gluteal muscle, the transgluteal approach for sciatic nerve entrapment has been used mostly in orthopedics8,10-12,16-18,24). The posterior hip approach, also known as the "Southern" or "Moore" approach in orthopedics11,12), is an approach to address the hip joint in the lateral decubitus position by splitting fibers of the gluteus maximus after incision in the fascia lata and iliotibial band and dissecting the piriformis and short hip external rotators. In this approach, the lateral tendinous portion of the piriformis muscle that is inserted into the greater trochanter is first cut and lifted. The piriformis muscle is then dissected to identify the underlying sciatic nerve24). Therefore, it is judged as a lateral approach to the sciatic nerve running medial from the greater trochanter.
On the other hand, the endoscopic approach, which has been recently introduced in the field of orthopedics, is considered to be a direct approach to DGS including sciatic nerve entrapment7,10). It has been reported that endoscopic surgery through three portals for peritrochanteric access can relieve the pathologies compressing the sciatic nerve such as the piriformis tendon, atypical fibrous band, and hamstring tendon7,10,16,18). However, endoscopic surgery is also basically considered as a lateral approach to access the peritrochanteric space from the side. Therefore, an endoscopic approach to access the deep gluteal space from the posterior side has also been introduced18).
The authors' transgluteal approach basically uses a transgluteal approach for the pudendal nerve located just medial to the sciatic nerve1,8,22). The pudendal nerve originating from the S2 to S4 sacral rami passes out of the pelvis through the infrapiriform notch of the greater sciatic foramen ventral to the sciatic nerve1). Common site of pudendal nerve entrapment is located between the sacrospinous ligament and STL at the level of the ischial spine1,2,8,22). This site is about 3 to 4-cm medial to where the sciatic nerve is compressed by the piriformis muscle at the greater sciatic notch (Fig. 1). Therefore, the area where the pudendal nerve runs under the STL corresponds to the area of the piriformis muscle exposed posteriorly by a transgluteal approach. The upper extent of our transgluteal decompression begins where the piriformis muscle passes through the lateral edge of the STL in the sciatic notch.
The STL positioned posteriorly and inferiorly in the pelvis is associated with stability of the sacroiliac joint23). It spans between the sacrum and the ischial tuberosity, forming posterior boundaries of the greater and lesser sciatic foramen (Fig. 1). The greater sciatic foramen is partly filled by the emerging piriformis muscle, above which the superior gluteal vessels and the nerve leave the pelvis23). Below it, the inferior gluteal vessels and nerve, internal pudendal vessels and nerve, sciatic and posterior femoral cutaneous nerve all leave the pelvis23). The piriformis muscle originates from the anterolateral surface of the sacrum and passes laterally and inferiorly through the greater sciatic foramen. Therefore, the piriformis muscle is supported posteriorly by the STL as it passes through the greater sciatic foramen (Fig. 1)6,23). The upper part of the pelvic surface of the STL is also a site of attachment for piriformis muscle similar to the lower fibers of the gluteus maximus6). Therefore, to completely remove the portion of the piriformis muscle compressing the sciatic nerve, the lateral margin of the STL to which the piriformis muscle is attached must be cut to check the piriformis and the sciatic nerve located below. This is especially important in surgery for Beaton and Anson's Type 3 sciatic nerve variation4), in which one division of the sciatic nerve descends anteriorly to the piriformis muscle and the other descends posteriorly. It is also required for sciatic nerve entrapment due to hypertrophy of the piriformis muscle4,13).
2. More Direct Neurosurgical Approaches and Our Method
A direct neurosurgical posterior approach for sciatic nerve entrapment has already been introduced by Filler6). They suggested a minimally-invasive, transgluteal approach via a 3-cm incision with tubular retractor system19). An excellent or good outcome was achieved by this approach in about 80% of patients19). If the same result could be obtained, the approach with a smaller incision is preferable. Filler6) have performed neuroplasty of the sciatic nerve after resection of the piriformis muscle. However, the authors always secured the sciatic nerve and its division first and then removed the piriformis muscle.
After splitting and traction the gluteus maximus muscle, we exposed the part where the piriformis muscle ran under the lateral margin of the STL. Unlike the approach of Filler6), the orientation of the sciatic nerve and its divisions within the subgluteal fat space, inferior to the piriformis muscle, was first addressed. The entrapping portion of the piriformis muscle and tendons were then removed. The inferior gluteal nerve and vessels must be secured through dissection of the subgluteal fat space so that the sciatic nerve from which they originated could be traced. In our approach, identification of the sciatic nerve is of utmost importance. The pathology of maximal entrapment can be confirmed by separating the sciatic nerve and the piriformis muscle located below the piriformis muscle.
About 15 cm of the sciatic nerve and its division were explored and decompressed, extending to and through the sciatic notch as well as distally along most of its course in the ischial tunnel. In Type 1 sciatic nerve entrapment4), both the bumpy portion of the piriformis muscle that puts pressure on the sciatic nerve and the lower edge of the tendon are removed. In Type 2 sciatic nerve entrapment, both the accessory piriformis muscle and tendons that are sandwiched between tibial and peroneal divisions of the sciatic nerve are removed in addition to the main piriformis muscle (Fig. 1). Therefore, a much larger portion of the piriformis muscle is removed from the sciatic nerve pathway than the approximately 2-cm segment of the piriformis muscle resection described in the prior minimal-invasive transgluteal approach19).
In summary, our transgluteal approach has several differences from the one proposed by Filler6). First, the decompression of the sciatic nerve is extended proximally to the greater sciatic notch. Second, the sciatic nerve is secured proximal by confirming the inferior gluteal nerve. Third, the piriformis muscle is removed at the end. Fourth, only the portion where the piriformis muscle encloses the sciatic nerve is excised.
3. Points to Note in Sciatic Nerve Decompression and Intraoperative Neurophysiology
The sciatic nerve has no external landmark in the hip. Therefore, the location of the incision is the most important. For direct posterior access to the sciatic nerve, it is most important to check the relationship between the femur head and the sciatic nerve in coronal MRI images. In addition, the predicted path must be marked on the hip using c-arm fluoroscopy.
The transgluteal approach to the sciatic nerve is known to be possible even using local anesthesia19). However, we performed general anesthesia for the standard transgluteal approach. Considering the patient’s pain and discomfort due to manipulation and retraction of the gluteus and piriformis muscles and tendons and the nerve dissection and the need for illumination of the deep surgical site, surgery under general anesthesia is thought to be more effective for complete and accurate decompression of the sciatic nerve and its branches than that under local anesthesia. In addition, intraoperative monitoring, especially intraoperative nerve stimulation, could be used to prevent unexpected nerve damage. Intraoperative nerve stimulation is important in surgery under general anesthesia to identify the inferior gluteal nerve at the initial stage of dissection and track it to accurately identify tibial and peroneal divisions of the sciatic nerve. In addition, hidden divisions can be quickly identified in the surgical field, which could help prevent nerve damage during surgery. Fig. 3 summarizes intraoperative stimulation responses of nerves to be checked during sciatic nerve entrapment. Somatotopy of the sciatic nerve course was confirmed.
4. Limitations
We acknowledge that our gluteal approach has a longer skin incision and more extensive dissection of the gluteal muscle than previously introduced minimally-invasive transgluteal approaches19). However, our surgical goal is to achieve circumferential decompression of the sciatic nerve and its divisions running from the sciatic notch to between the sciatic tunnel. Comprehensive visual identification of the sciatic nerve is important to confirm the exact compression site and pathological findings by the piriformis muscle and determine the extent of muscles and tendons to be removed for circumferential decompression. This is thought to be particularly important for inexperienced surgeons or planning for sciatic nerve decompression for the first time. Therefore, a transgluteal approach that can accurately expose the decompression area is thought to be helpful in reducing the risk of unwanted nerve damage and enabling circumferential anatomical decompression.
Since results of sciatic nerve entrapment using our transgluteal approach have not yet been reported, it is difficult to compare them with the existing orthopedic approach. However, from our perspective of circumferential decompression of the sciatic nerve, there are parts that are difficult to understand in previous reports. For example, the fibrous band compressing the sciatic nerve7,16-18), sometimes described as endoscopic sciatic nerve decompression, appears to be irresponsible from our point of view. Unless these fibrous bands are caused by some trauma or surgery, it is thought that it would be difficult to solve the entrapment of the sciatic nerve simply by endoscopic dissection of the sciatic nerve. Additional findings will be presented when results of the transgluteal approach for sciatic nerve entrapment are summarized in the near future.
CONCLUSION
There are several variations of the transgluteal approach to sciatic nerve entrapment. The authors presented a surgical technique that allows direct posterior access to the area where sciatic nerve entrapment occurs by the piriformis muscle and STL. Comprehensive, circumferential decompression of the sciatic nerve is thought to be possible through our more proximal approach including the lateral margin of the STL. In addition, intraoperative electrical stimulation of the sciatic nerve, its divisions, and the inferior gluteal nerve can prevent nerve damage and aid in orientation during surgery.