INTRODUCTION
Neurogenic thoracic outlet syndrome (NTOS) is a recognized condition resulting from insufficient space surrounding the brachial plexus. Multiple anatomical structures may compress the brachial plexus; recent findings indicate that subclavius muscle compression during shoulder abduction may also contribute. Specifically, subclavius muscle hypertrophy in overhead athletes may lead to neuronal structure compression. We present a case in which successful treatment of NTOS was achieved through addressing subclavius muscle hypertrophy.
CASE REPORT
A 41-year-old male visited the hospital with functional disorders, including pain, numbness, abnormal sensation, and right shoulder weakness. The pain and numbness were primarily located around the shoulder not along with any sensory dermatome, with the main symptom being a pain in shoulder abduction and flexion position. The patient mentioned that the symptoms listed above had been gradually worsening for the past three months. He experienced sudden right shoulder pain and tingling sensation, leading to multiple hospital visits. Persistent symptoms brought him to our hospital. The patient had no relevant medical history and had been working as a heavy goods delivery worker for 10 years. Initial physical examination showed no right shoulder muscle atrophy or skin abnormalities, such as rashes or discoloration. Neurological examination revealed muscle strength was reduced to grade IV in right shoulder flexion and abduction, and there was end-range pain during passive range of motion, but a whole range was achievable. Furthermore, there was no motor weakness or sensory changes at the distal finger and wrist level, and the scapular area appeared normal, with no abnormal findings such as winged scapula observed., with severe pain (visual analogue scale [VAS] score 8) and radiating pain in the right upper extremity during shoulder flexion and abduction. A cervical spine magnetic resonance imaging (MRI) showed no abnormalities causing radiculopathy or myelopathy. X-ray and computed tomgoraphy imaging of the cervicothoracic spine and chest confirmed no clavicle or first rib deformities. Contrast-enhanced MRI was performed to explore the brachial plexus area, generating axial, coronal, and sagittal images and comparing anatomical neutral position and right shoulder abduction to verify potential brachial plexus compression.
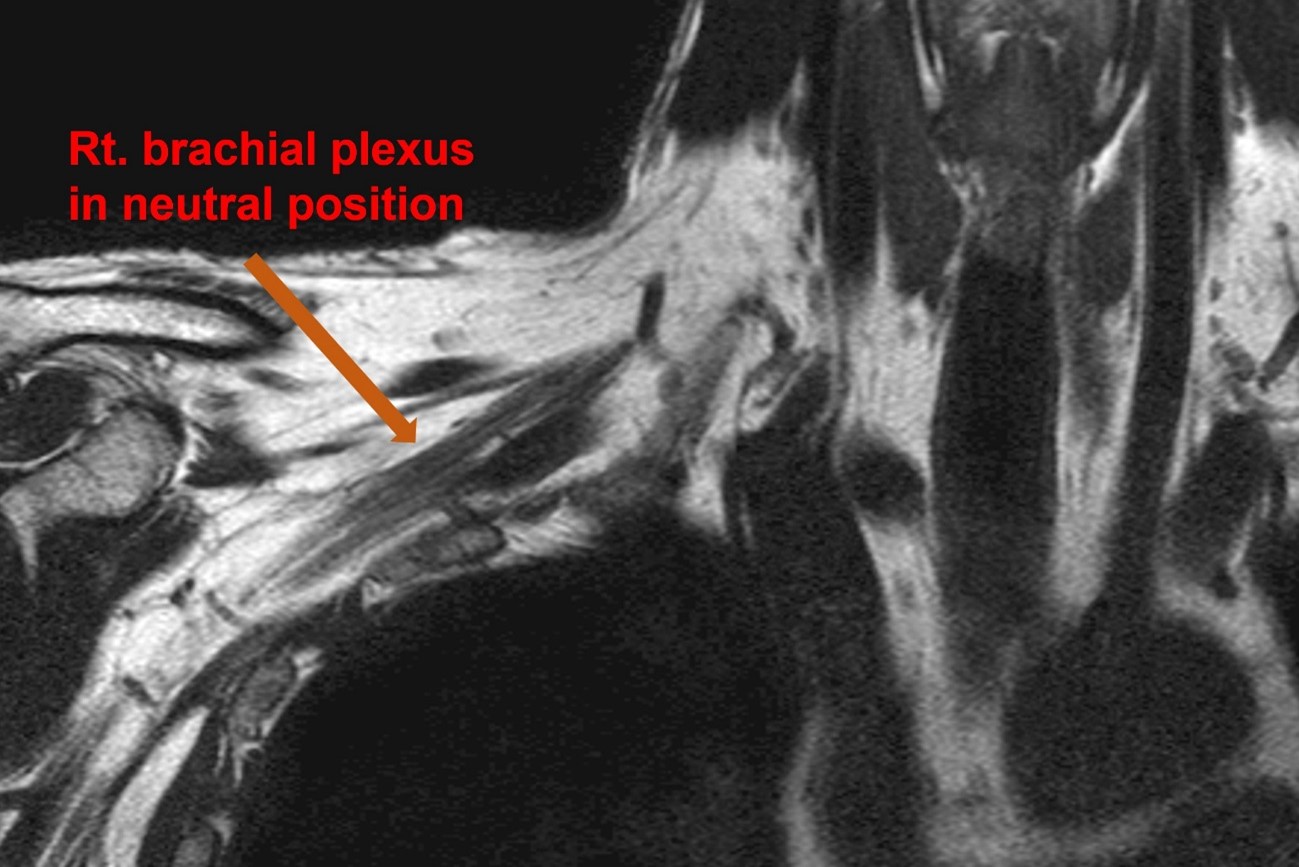
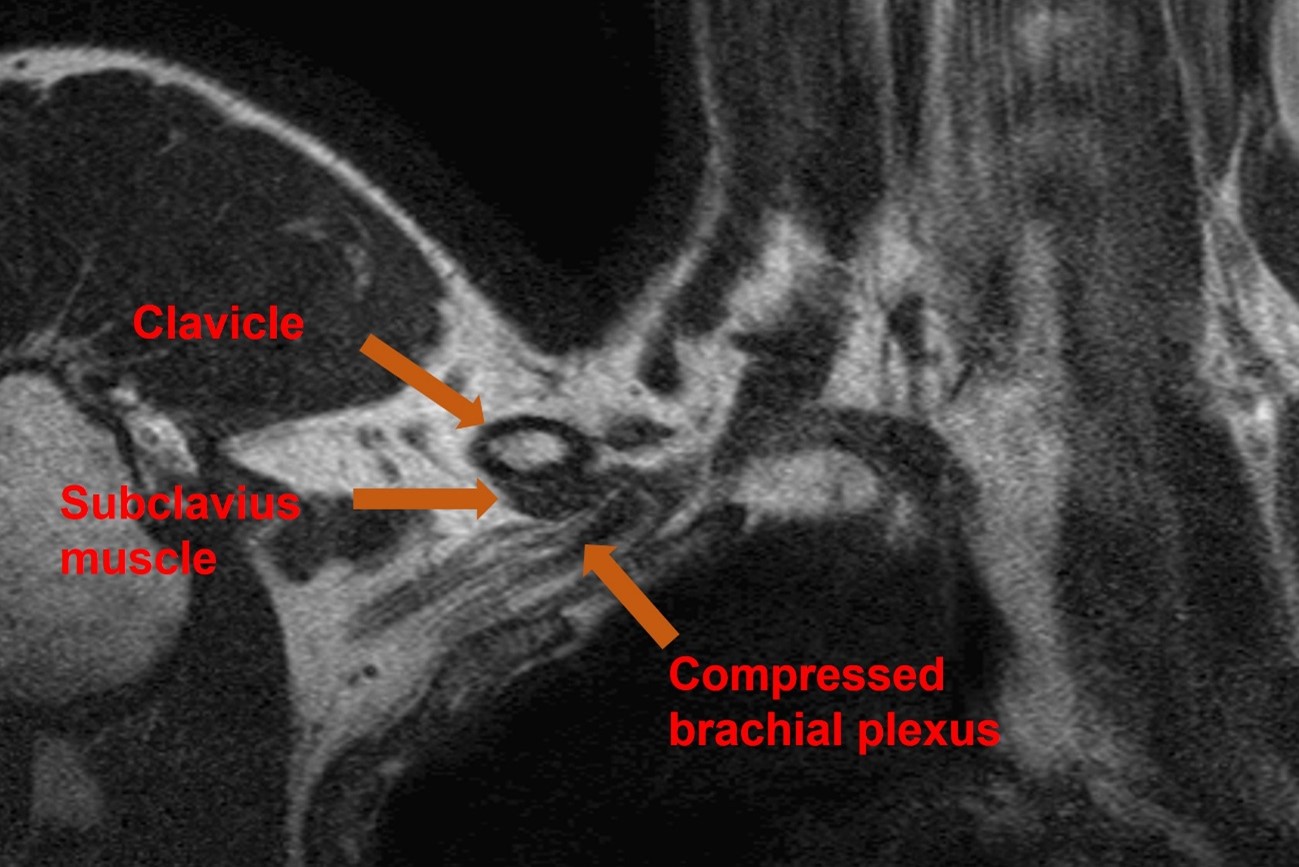
MRI results revealed no contact between the brachial plexus and subclavius muscle in the anatomical neutral position (Fig. 1). However, a high-intensity signal was identified in the image taken at the right shoulder abduction position, indicating reduced fat tissue density around the nerve due to subclavius muscle compression. Additionally, reduced right subclavian artery diameter and collapsed right subclavian vein were observed (Fig. 2).
After symptom onset, conservative treatment was administered for six weeks, followed by an electrophysiological examination, revealing right brachial plexopathy at the medial cord or lower trunk level and partial axonal injury. Despite treatment, the patient continued experiencing shoulder weakness (grade IV), severe radiating pain, and numbness. Surgery was scheduled two months after symptom onset.
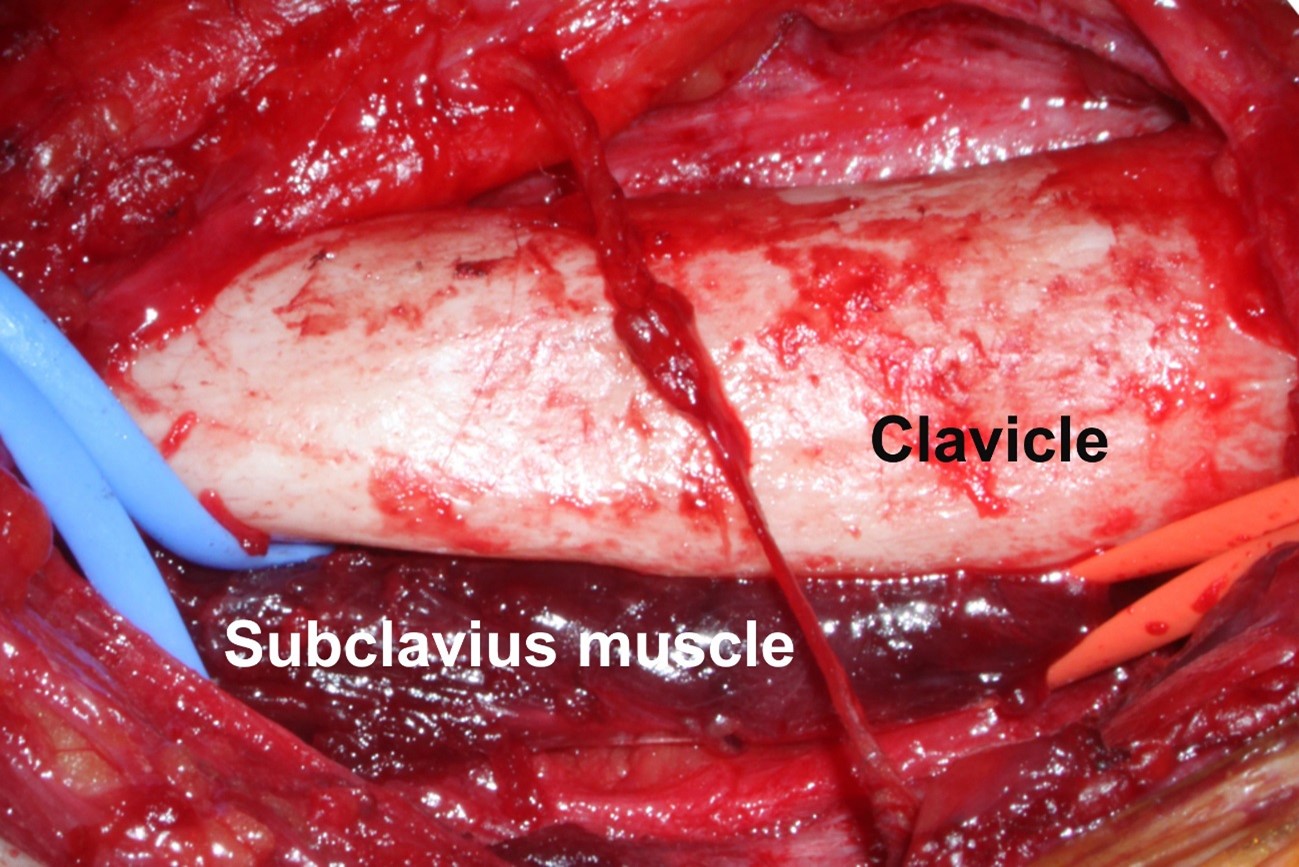
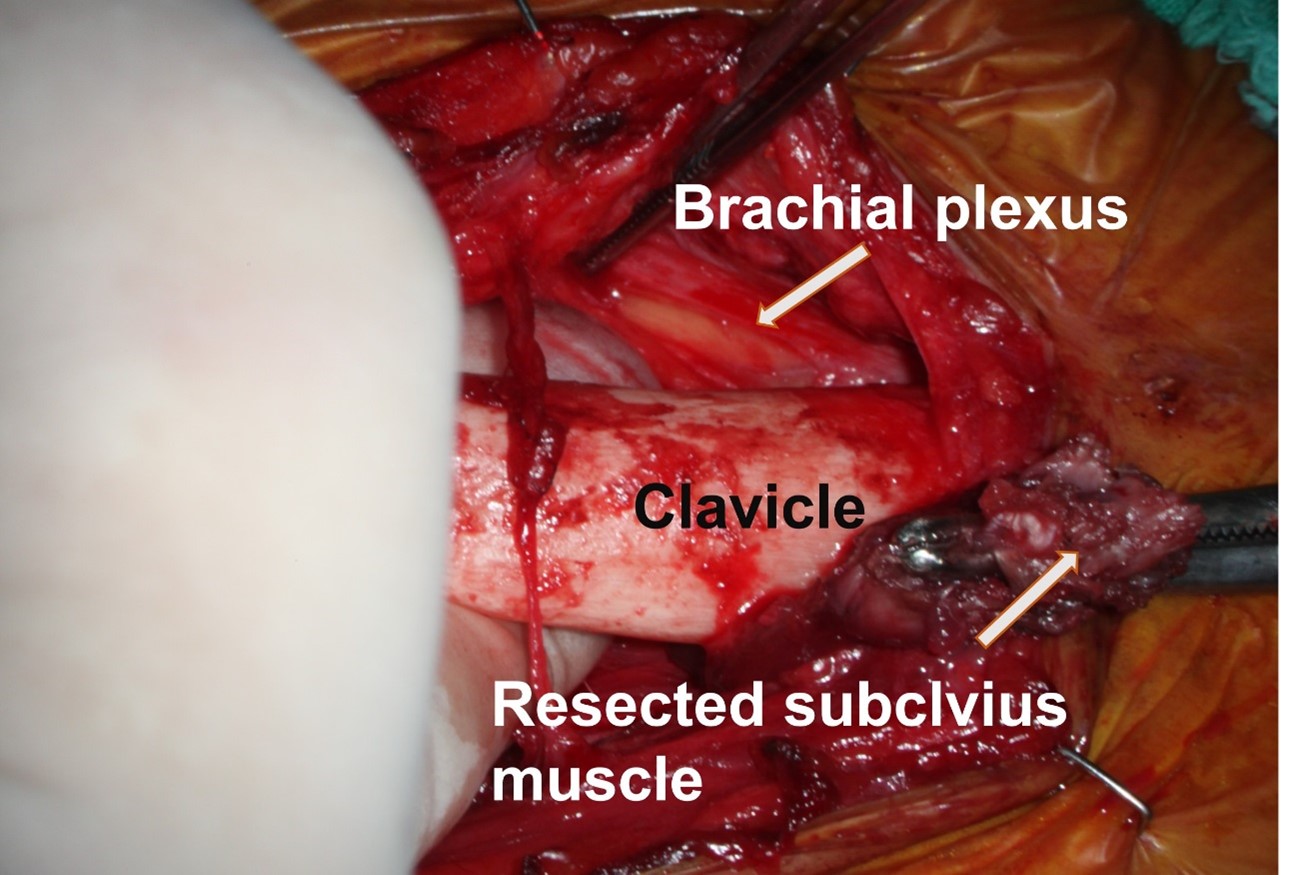
Under general anesthesia, the patient was placed in a supine position, and a paraclavicular approach was chosen with a 10 cm horizontal skin incision around the clavicle to decompress the brachial plexus in the subclavian area. A hypertrophic subclavius muscle was identified below the clavicle, along with structures like the artery, vein, and compressed brachial plexus. Fine dissection and careful coagulation were performed to expose both the origin and insertion site of the subclavius muscle using Metzenbaum scissors and a bipolar coagulator (Fig. 3). It was confirmed that there was no damage to the surrounding artery, vein, or nerve. The origin and insertion site of the subclavius muscle were clearly identified, and the final resection was done using a monopolar coagulator for cutting and coagulation. Upon examination with a microscope during surgery, it was confirmed that the compressed brachial plexus nerve was expanded and decompressed. The subclavius muscle was completely resected, and the subclavicular area became abundant. The space was large enough for finger exploration, and it was possible to confirm the expansion of the previously compressed brachial plexus (Fig. 4). No abnormalities were found in other structures compressing the brachial plexus. First rib resection and anterior scalene muscle (ASM) release were not performed.
Post-surgery, the patient wore a shoulder brace, and a follow-up MRI was conducted one week later to confirm changes. Compared to preoperative MRI, perineural fat obliteration around the brachial plexus was recovered, and subclavian artery diameter reduction and subclavian vein collapse improved (Fig. 5). The patient was discharged two weeks after surgery, reporting significant numbness improvement. Three months after surgery, physical examination showed dramatic right shoulder muscle strength improvement (grade V) and no severe pain during shoulder abduction (VAS 1). Follow-up electrophysiological examination confirmed the disappearance of upper extremity muscle degeneration potential.
DISCUSSION
Thoracic outlet syndrome (TOS) was initially described in 1927 by Adson and Coffey1), who coined the term ‘scalenus anticus syndrome’ and suggested that symptoms were caused by the compression of the subclavian artery by the ASM. TOS is currently defined as the compression of the brachial plexus, subclavian artery or vein, or the invasion of the brachial plexus in three distinct areas: the scalene triangle, costoclavicular space, and subcoracoid (pectoralis minor) space13,19). Additionally, a report has documented non-specific TOS types also15).
Neurogenic TOS is differentiated from vascular TOS based on clinical presentations and symptoms12). Neurogenic TOS was characterized by pain, weakness, and paresthesia of the upper extremity, while vascular TOS was primarily characterized by symptoms of arterial or venous insufficiency such as coldness, cyanosis, and edema. In addition, vascular TOS patients tended to have a history of trauma, while neurogenic TOS patients were more likely to have repetitive strain injuries or other occupational factors.
Recently, standardized clinical diagnostic criteria for neurogenic thoracic outlet syndrome have been published, leading to increased awareness of this condition10). Two large-scale studies demonstrated that over 90% of NTOS cases result from neural compression on the brachial plexus at the C5 to T1 levels8,18). First rib resection following standard surgical procedures has an approximate success rate of 90%9,17).
The electrophysiological study results showed axonal injury of the lower trunk or medial cord, which may not fit well with the case patient's symptoms of decreased shoulder strength. However, the dynamic MRI results demonstrated brachial plexus compression due to subclavius muscle hypertrophy, causing symptoms limited to the right shoulder. We believe the decrease in shoulder motor strength is due to NTOS, as supported by the MRI findings. Additionally, it is believed that the finding that appeared preoperatively on the electrophysiological study and then disappeared was a secondary finding caused by the hypertrophied subclavius muscle mechanically irritating the nerve. We believe that the hypertrophy of the subclavius muscle exacerbates the compression and irritation of a portion of the brachial plexus in the narrow costoclavicular area during shoulder abduction or flexion. This is thought to have caused severe numbness and pain, which then led to a secondary reduction in muscle strength.
When selecting surgical procedures for NTOS, trans-axillary, superior clavicular, or supraclavicular approaches combined with infraclavicular approaches are typically considered. Before surgery, a thorough review of these three options is necessary. Distinguishing between NTOS and vascular TOS is also necessary too. A comprehensive assessment of the brachial plexus's surrounding structures and their compression degree should precede the surgical approach determination. In some instances, wide resection, including the first rib, may be required.
On the other hand, there have been several reports that the subclavius posticus muscle can contribute to thoracic outlet syndrome2,3,6,7,14,16). The connection between subclavius muscle hypertrophy and TOS has been investigated in multiple cadaveric studies5,11). The subclavius muscle's origin is the first rib and its costal cartilage, while its insertion is the subclavian groove. The muscle is known to cause clavicular depression and first rib elevation. One study reported that adding subclavius muscle resection to NTOS palliative treatment could improve results13). Another study suggested that botulinum toxin injections into the subclavius muscle could serve as a potential TOS treatment option4).
Diagnostic technology advancements have enabled more detailed radiological evaluations of anatomical structures compressing the brachial plexus. In this case, preoperative MRI revealed brachial plexus compression due to subclavius muscle hypertrophy, causing symptoms limited to the right shoulder. Based on this finding, we planned right subclavius muscle decompression only, yielding a favorable outcome.