INTRODUCTION
Congenital kyphosis is a rare congenital deformity caused by developmental anomalies that impair longitudinal growth and vertebral rotation in the sagittal axis [10]. It often causes uncontrolled pain and severe neurologic deficits in pediatric patients, which are frequently aggravated by the adolescent growth spurt.
Corrective surgery for congenital kyphosis involving upper thoracic region is challenging; intra-operative and post-operative complications include neurologic deterioration and mortality due to limitations such as invisible spine imaging on X-rays, proximal fixation points including cervical spine, and vulnerable spinal cord in this area. Thus, surgical procedures should be carefully planned to minimize risk. Posterior vertebral column resection (PVCR) technique has an advantage of allowing both anterior and posterior manipulations from a single approach [15], but the reports regarding its application on pediatric patients are rare. We present a case of congenital kyphosis of the upper thoracic region treated with PVCR to share lessens we have learned.
CASE REPORT
1. History and examination
A 12-year-old male from Mongolia with no known medical history presented with progressive gait disturbance and kyphotic deformity of the cervicothoracic junction that had rapidly progressed in the last 2 years. At the time of the admission, the patient complained of severe upper back pain, and his neurologic status was determined to be category C on the American Spinal Injury Association Impairment Scale [8]; he exhibited urinary urgency and constipation, and rigidity in both legs, causing him to be dependent on walker support during ambulation. On spine X-rays, cervical lordosis (determined by the C2-C7 Cobb angle) was measured at 70.3°, thoracic kyphosis (determined by the T1-T12 Cobb angle) was 47.3°, lumbar lordosis (determined by the L1-L5 Cobb angle) was -18.5°, and the C7-T6 Cobb angle was 64.2° (Fig. 1). Three-dimensional computed tomography revealed anterior and medial aplasia in the T2-T4 vertebrae and anterior hypoplasia in T1 and T5, indicating type 1 deformity. Also, the patient’s pulmonary function was compromised due to pectus carinatum.
2. PVCR
The patient received PVCR of T1-2-3-4-5, posterior screw fixations of C5-6-7-T6-7-8, and posterolateral interbody fusion with autobone. As the operation began, trans-4-aminomethylcyclohexane-1-carboxylic acid (TXA) was applied to reduce intraoperative bleeding by immediately giving 500 mg TXA intravenously followed by dripping a TXA solution at 5 mg/kg/h. After meticulous dissection, resection of the transverse processes and rib heads of T2-T5 was followed by laminectomies of T1, 2, 3, 4, and 5. Pedicle screws were inserted on each side of the vertebrae using the free-hand technique because intraoperative fluoroscopic guidance was not useful for defining the exact anatomy of the cervicothoracic junction. Temporary rods were assembled on the opposite side to provide structural stability during the resection. The vertebral body resection was performed from the lateral to the medial direction, after which the temporary rod was removed and placed on the other side. The resection was repeated on the opposite side. The midline bridging bone of the posterior part of the vertebral body just ventral to the spinal cord was removed with gentle traction of the spinal cord. Finally, the rods were placed on both sides, and the wound was closed. Total operation time was 529 min, and blood loss totaled 2,700 mL. Intra-operative neurophysiologic monitoring (IONM) with motor-evoked potentials (MEPs) was implemented, but we were unable to acquire signals from the lower extremities at any point in the operation.
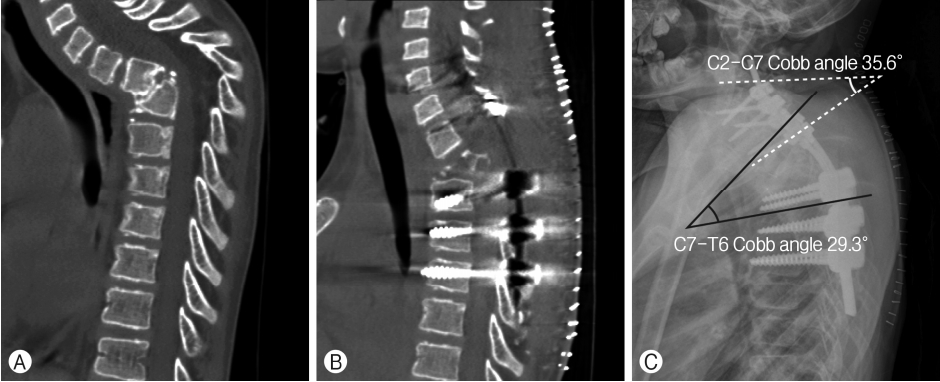
The patient was admitted to the intensive care unit after surgery and was moved to the general ward the day after. A Foley catheter was removed a week after the operation so that he could self-void; the patient’s weakness in the lower limbs improved considerably such that he was able to walk with an assist walker 2 weeks after surgery. There were notable improvements in radiologic parameters: cervical lordosis improved to 35.6°, and Cobb angle of C7-T6, 29.3° (Fig. 2). Cervicothoracic X-rays were taken at a Mongolian hospital 75 days after the operation to show the instrumentations and the sagittal alignment of the spine were well maintained, with the cervical lordosis of 34.5° and the C7-T6 Cobb angle of 28.5° (Fig. 3). The patient was able to walk with a cane 7 months after the operation.
DISCUSSION
Correction of a moderate spinal deformity can be effectively and safely performed from posterior, anterior, or posterior and anterior approaches [1,5,13]. Winter and Hall [18] argued that severe deformity with thoracic kyphotic angle >60° and neurologic deficiency required surgical interventions from both anterior and posterior approaches to achieve adequate decompression and support of the structure. It is thought, however, that instrumentation without osteotomy may not allow sufficient correction for severe kyphosis; often, conventional osteotomy techniques such as Smith-Peterson osteotomy or pedicle subtraction osteotomy do not yield the desired correction. Moreover, a surgery requiring both anterior and posterior approach can be complicated by excessive intraoperative blood loss, a long operation time, and a manipulation of the thoracic cavity which increases a risk of respiratory complications. PVCR is a surgical method that can address these issues. In 2002, Suk et al. [15] introduced PVCR in an attempt to reduce the surgical complications and technical difficulties of VCR from simultaneous anterior and posterior approaches. Although it can cause lethal complications and is also technically challenging, PVCR offers several advantages. It allows both anterior and posterior column manipulation through a single posterior approach and yields a higher degree of deformity correction. In addition, PVCR helps preserve pulmonary function because the thoracic cavity is not involved. Ozturk et al. [12] reported an average Cobb angle correction rate of 62%. Yang et al. [20] reported a mean correction of 58.9° and a correction rate of 63.1% in patients with kyphosis. Using PVCR, we could correct the patient’s severe kyphosis while reducing operation time and blood loss, without opening the thoracic cage.
In a spinal deformity correction surgery, massive intraoperative bleeding may occur as it frequently involves long level osteotomies and instrumentations. An extensive blood loss often necessitates transfusion, which can potentially cause postoperative complications such as pulmonary edema, hemolytic and non-hemolytic transfusion reactions [17], and wound infections [6]. Furthermore, the upper thoracic region is at a higher risk of spinal cord infarction during a spinal deformity surgery due to the inadequate collateral supply. Thus, during a corrective surgery for a spinal kyphosis, a surgeon must exploit all possible blood conservation strategies, one of which is the intra-operative use of TXA. There have been several studies advocating the efficacy of TXA in reducing intraoperative blood loss and the necessity of post-operative blood transfusion [11,19]. Choi and his colleagues [3] argued that the use of TXA could effectively lower surgical bleeding, intra-operative transfusion requirements, and pos-toperative transfusion volume in patients receiving spinal deformity surgeries involving at least 5 vertebral levels. In addition to use of TXA, pre-operative intravenous ferric carboxymaltose infusion should be considered to reduce the need for blood transfusion and improve outcomes.
We encountered a few challenges during the operation. Although kyphosis in the upper thoracic spine with a kyphotic apex above T5 is uncommon, it is frequently accompanied by more serious neurological deficits [9,10]. A complete removal of the midline bridging bone of the vertebral body required the utmost attention, as too much traction of the thoracic cord would cause neurologic impairments. For the same reason, hemostasis of the epidural bleeding was dangerous.
IONM is considered mandatory for any patient with congenital deformity undergoing a corrective surgery. There is a higher risk of post-operative paraplegia in patients with congenital spinal deformities than other causes of spinal deformities [9]. MEPs are known to be most sensitive to iatrogenic damages to the spinal cord and nerve roots [14], and their changes can occur due to hypotension, extreme manipulation of the cord, and osteotomy gap closing. However, in the presented case, intraoperative MEPs failed to detect any signal since the beginning of the surgery. We could find few publications that reported IONM failure in pediatric scoliosis patients with severe cerebral palsy [4], but the reasons for the monitoring failure remain to be further analyzed. We assume that IONM signals sometimes cannot be acquired in cases of severe deformity with neurologic deficits. One may consider awake surgery under local anesthesia as done in patients with multiple comorbidities if patients can tolerate [2,7]. However, this may not always be feasible in pediatric patients who are less likely to cooperate well during the awake surgery.
Multilevel cervical fixation might be required in patients with kyphotic apex at upper thoracic spine, and it is of considerable difficulty especially in pediatric patients. In our case, we suspected that lateral mass of the patient was too small to endure corrective stress of screw fixation after surgery or the cantilever procedures during intra-operative correction, so we decided to insert cervical pedicle screws. An intra-operative C-arm X-ray device could not be utilized for the screw insertion in the cervicothoracic junction because of bone and soft tissue in the shoulder region. It is obviously more challenging to accurately insert screws in a deformed spine than in a spine with a normal anatomy. Intra-operative navigation using intraoperative computed scan or reformatted image of cervical and thoracic could be considered as one of the solutions, although it is not quite popular in our daily practice [16].
There are a few limitations to this case report. First of all, a longer follow-up period is necessary to evaluate the change of the patient’s structural and neurologic status, as the bones are immature and ligaments are elastic during adolescent ages. We were able to confirm the neurologic improvements and radiological stability 7 months after the operation when we visited Mongolia, but a regular follow-up of the patient was practically impossible. Second, we need to collect and analyze more thoracic kyphosis cases to be able to address technical difficulties and solutions associated with PVCR in patients with congenital kyphosis.
Congenital kyphosis in the upper thoracic region may cause devastating consequences. PVCR is an effective surgical method for correcting severe kyphosis, allowing greater correction of the deformity angle, reduced operation time and blood loss. Since PVCR is a demanding procedure, surgeons must carefully analyze a case preoperatively and establish a detailed surgical plan.