INTRODUCTION
Acute subdural hematoma (ASDH) usually results from traumatic brain injury (TBI) and occurs in 12% to 30% of patients with severe head injury [18]. A recent study suggested that the incidence has increased from 6.67/100,000 to 14.7/100,000 between 1993 and 2006 among US populations, and the cost to treat has increased 67% during that same period [9], which could present growing socioeconomic problems for patients with ASDH. It often results in neurologic deterioration and/or intracranial hypertension, requiring emergency decompression surgery for most patients [4]. Patients with neurological deficits and signs of increased intracranial pressure (IICP) are considered for surgery, and they hold a high mortality rate, generally 40% to 70% in the literature depending on existing clinical factors such as the level of consciousness [4,6,9]. Since ASDH with severe mass effect and neurologic symptoms almost always undergo immediate decompressive surgery, the observation of its natural clinical course is restricted to patients chosen for conservative treatment. There have been reported cases where the rapid resolution of ASDH showing neurological improvements with conservative treatment [1-3,5,8,10,12,14,15,17,19-22]. Here, we report a case of ASDH with severe mass effect by hematoma subject to immediate surgery that showed gradual neurological progress after 8 hr of admission and spontaneous resolution within 4 days after TBI. The possible proposed mechanism of the resolution of hematoma will also be discussed.
CASE REPORT
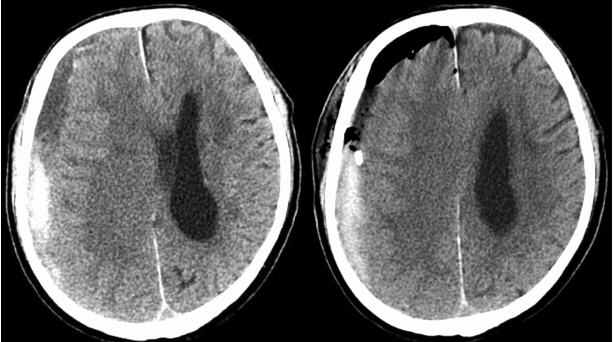
A 74-year-old male was admitted to our emergency room (ER) after slipping down in the bathroom. In 2009, he received cardiac valve replacement surgery for aortic valve stenosis and regurgitation and mitral valve regurgitation with atrial fibrillation and was on warfarin ever since. He was stuporous on admission with Glasgow Coma Scale (GCS) of E1V2M4. Initial brain computed tomography (CT) suggested a thick right frontotemporal ASDH shifting the right brain parenchyma to the left with subfalcine and uncal herniations (Fig. 1A). Immediate surgical intervention was considered as a first option of treatment. However, the family claimed that the patient held strong principles against any aggressive treatment with extensive general anesthesia and refused the surgery to honor his wishes. His respiration became progressively shallow but the family also refused endotracheal intubation.
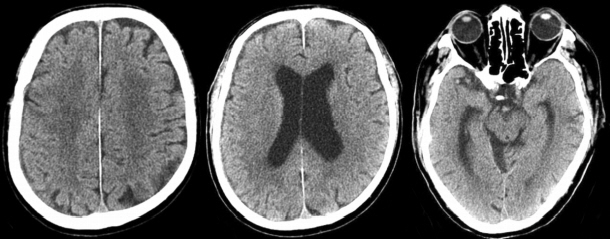
He was admitted to the intensive care unit for close observation under medical treatment for ICP control. About 8 hr later, during medical treatment, his consciousness became drowsy with GCS of E3V4M6, and the follow-up CT indicated slight signs of reduced amount of hematoma and partial restoration of the midline shift (Fig. 1B). His neurologic symptoms improved progressively and a brain CT taken approximately 4 days later showed a significant spontaneous reduction of hematoma with improved of midline shifting and herniation (Fig. 1C). Eventually, the patient developed a chronic SDH (CSDH) that was simply drained via burr-hole trephination (Fig. 2). He was discharged on the 20th day of admission and able to return to his daily social activities with Karnofsky Performance Scale of 100 at about 3 months postdischarge. The follow-up brain CT showed a nearly complete resolution of SDH along the right cerebral convexity (Fig. 3).
DISCUSSION
It is generally accepted that ASDH with neurologic deficits and radiographically indicating severe brain injury calls for immediate surgical interventions such as decompressive craniectomy due to its fast lethal clinical course [4]. However, there could be situations in the clinical field where surgical intervention is not performed for various reasons such as poor initial medical status and family wishes or a patient’s will. Several case reports have shown patients whose ASDH resolved rapidly and spontaneously within hr to days with good clinical outcomes, as demonstrated by CT [1-3,5,8,10,12,14,15,17,19-22]. We report a rare case of ASDH with a significant midline shift that resolved spontaneously under conservative treatment.
A simple ASDH with moderate thickness and visible “low-density band” between the hematoma and inner table of the skull on CT could be an indicator of the spontaneous resolution of hematoma, as suggested by other authors [2,8,12,14,17,19,21,22]. Other factors such as brain atrophy and coagulopathy due to previous medical conditions could also be responsible for spontaneous resolution (Table 1). Such spontaneous resolution phenomena can be explained as a dilution of the hematoma by cerebrospinal fluid (CSF) that has leaked from a tear in the arachnoid membrane leading to a washout of blood products with increasing brain swelling and increased IICP [16]. According to a review of adult cases on the spontaneous resolution of ASDH with mass effect, the most frequently mentioned factor to explain the disappearance of hematoma was the presence of a “low-density band” in CT (Table 1). Watanabe et al. [21] reviewed a case of an 88-year-old woman in a coma with ASDH who showed rapid resolution on CT and magnetic resonance imaging (MRI). Her consciousness steadily recovered to a GCS score of E2V4M5, and the follow-up brain CT revealed the spontaneous resolution of the hematoma and brain MRI showed a redistribution of hematoma to the supratentorial subdural space. Eventually, the patient developed CSDH 3 weeks later and a simple drainage was performed for evacuation. The author suggested that CSF had diluted the hematoma, which can be presumed from the “low-density band” on CT and that the presence of a wide subdural space due to brain atrophy from dementia might have caused the spontaneous resolution.
In our case, a “low-density” band was visible in the patient’s CT taken at ER (Fig. 1A) and the follow-up CT images showed that the hematoma resolved around that band first (Fig. 1B, C). The laboratory evidence of coagulopathy with international normalized ratio prolongation might have played a role, since the patient was taking warfarin for his heart condition, eliciting liquefaction of the hematoma and may have promoted redistribution. In addition, the presence of brain atrophy due to his previous history of cerebral infarction and old age might have rendered some space to compensate for the acute IICP before brain herniation began, as a similar phenomenon suggested by other cases [2,5,12,17,20,21].
It has been suggested that the use of antiplatelet agents prior to head injury could increase the probability of rapid resolution. Fujimoto et al. [7] reviewed 366 patients in total with ASDH using univariate and multivariate logistic regression analyses to identify predictors for rapid spontaneous resolution. In his study, the pre-hospital use of antiplatelet agents and the presence of a low-density band between the hematoma and inner skull bone on initial CT could be associated with liquefaction of the hematoma, thus encouraging rapid spontaneous resolution by facilitating redistribution with brain swelling. Other studies also supported this hypothesis, although brain atrophy instead of brain swelling is suggested as a main contributor in the process of dilution and redistribution [2,20].
Other hypotheses deal with a redistribution of hematoma and its products, caused by either brain swelling leading to IICP or further bleeding from the site [11,13,15]. In 1989, Niikawa et al. [15] reported that the dilution by CSF may be responsible for the rapid resolution of SDH via washing out or redistribution, and acute brain swelling might have triggered the pressure-induced redistribution of the ASDH. Another possible mechanism of the resolution could be a redistribution of the hematoma into other subdural or extracranial spaces through a fracture site of the skull [3]. Berker et al. [3] explained that such a process, in turn, could have triggered tears in the arachnoid membrane, thus washing out the hematoma by CSF. However, our case did not present with a definite skull fracture site or hemorrhages in other subdural spaces, making this less likely.
CONCLUSION
Although immediate surgical intervention is generally accepted as a golden standard for the treatment of ASDH with severe neurological progress, neurosurgeons must be aware that hematoma can resolve spontaneously in rare circumstances. When patients hold a high operative risk of taking anticoagulants with a visible “low-density band” in the brain CT and are very old, their guardians must be informed of the potential for spontaneous resolution. However, surgical decompression should remain the treatment of choice in ASDH with neurologic deficits and severe midline shift.