INTRODUCTION
Delirium is characterized by an acute fluctuating impairment of consciousness accompanied by disturbances in attention, cognition, and perception23,25). Postoperative delirium is a common complication of surgical procedures in the elderly, leading to difficulty in their postoperative care13,26). Additionally, patients with delirium are at risk of developing dangerous complications, such as falls, aspiration pneumonia, and accidental removal of lines and tubes in the hospital9). Delirium has been associated with prolonged hospital stays after elective surgery, increased medical expenditures, and a higher risk of readmission2,20). Therefore, identifying the possible risk factors for postoperative delirium may be helpful for its prevention.
Postoperative delirium has many probable risk factors, and there is controversy over the risk factors. The fixed risk factors include advanced age, pre-existing psychiatric disease, and the presence of multiple comorbidities. Among these, old age is the most strongly identified risk factor16). A number of reviews regarding postoperative delirium in general surgery, hip fracture surgery, and cardiovascular surgery have been reported5,25,30). However, there is currently still lacking of understanding of postoperative delirium after spine surgery, and the risk factors have not been fully elucidated, compared with other types of postoperative delirium.
The purpose of the present study was to assess the incidence and risk factors leading to postoperative delirium after elective spine surgery. This study was performed in an age-matched cohort to exclude well-established risk factors, older age.
MATERIALS AND METHODS
1. Study Design and Population
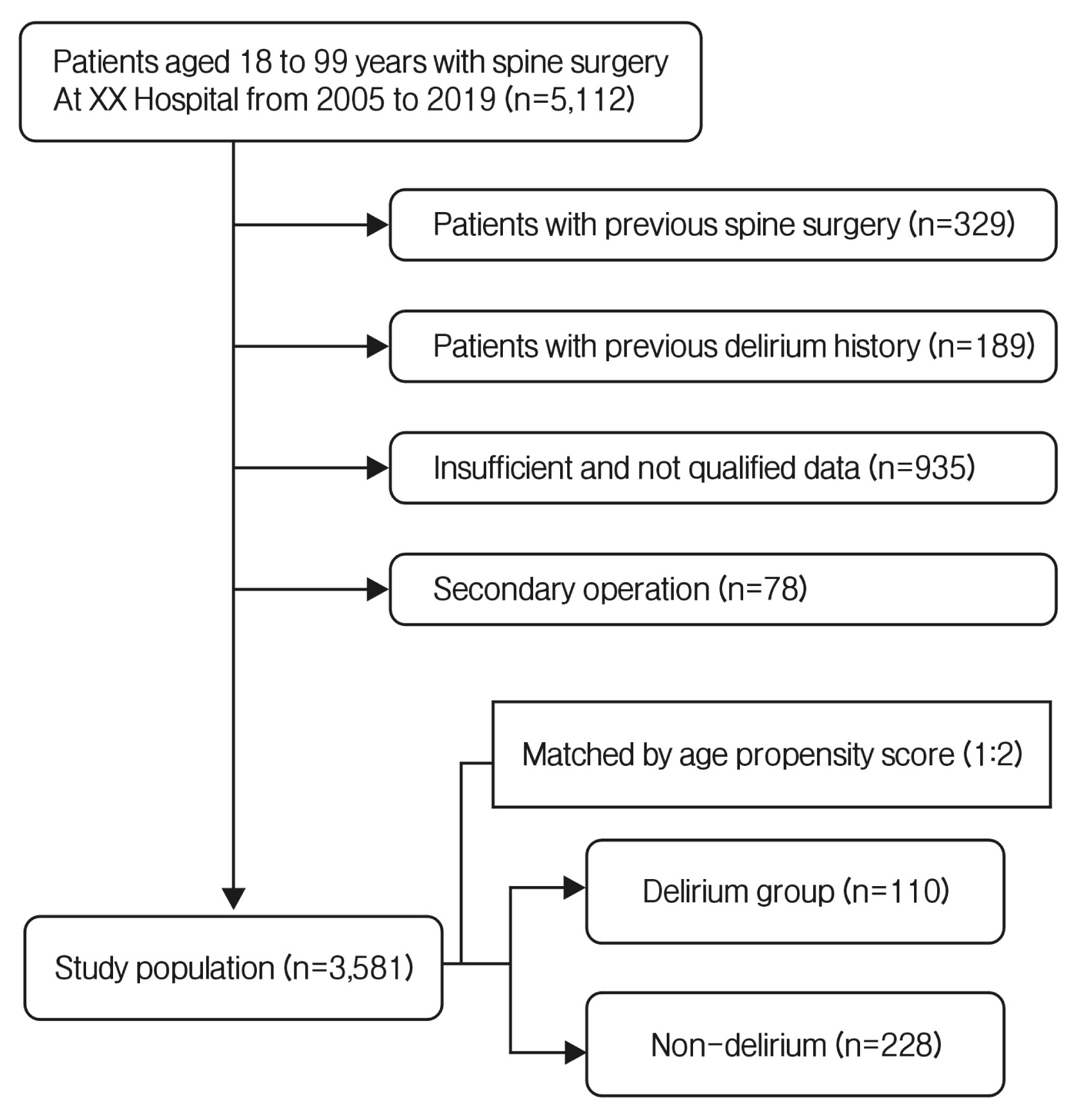
This study reviewed the incidence of delirium in 5,112 patients who underwent spine surgery for the first time under general anesthesia using inhalants, intravenous agents, or neuromuscular agents at Kangbuk Samsung Hospital from 2005 to 2019. Patients with a previous history of spine surgery or delirium, those with insufficiently and inappropriately recorded data in the electronic medical record (EMR), and those undergoing a reoperation, such as a hematoma removal or dural repair, at the same site were excluded. The study was approved by the Institutional Review Board (IRB) at Kangbuk Samsung Hospital (IRB approval no. 2020-06-041).
This study retrospectively reviewed the patient history for unmodifiable and modifiable factors in the past, the blood lab findings before and after surgery, and intraoperative factors. The blood analysis findings of the patients performed on the first, the second, and the third day of admission and postoperative day (POD) were reviewed for differences before and after the episode of delirium. The cases with missing values or outliers were excluded from this analysis
All of the included patients were divided into 2 groups, the delirium group and the non-delirium group. Statistical analyses were performed to calculate the incidence of delirium in all patients of both groups and the age-matched delirium and non-delirium groups of patients.
2. Assessment of Delirium
The period of delirium observation was predetermined as POD 0 to POD 3 for all patients. The incidence of delirium was determined according to the criteria described in the Diagnostic and Statistical Manual of Mental Disorders (DSM-V criteria)1), which is considered the gold standard for psychiatric evaluation. The nurses in the ward were educated to observe for symptoms of delirium, such as disturbances in cognition, attention and alertness, and notify when such symptoms were found. All the patients underwent psychiatric department consultation to confirm the diagnosis of delirium and were treated with medication prescribed by the department. The data regarding whether or not delirium occurred were stored in the EMR. In this study, delirium patients were identified based on their EMR data that showed the use of medication for delirium.
3. Statistical Analysis
The incidence of delirium was calculated according to the presence or absence of delirium after surgery (Table 1). The exclusion of patients was carried out, as shown in Figure 1. Each patient in the delirium group was age-matched with 2 patients in the delirium-negative group (age-matched, non-delirium group). In detail, 2 patients of the same age were selected at random. If that was not feasible, 2 patients were selected by widening the range by 2 years. Propensity score matching was performed using the principle of logistic regression. The delirium group subjects were matched with non-delirium group subjects with the allocated propensity score. Patients in the non-delirium group were selected using the Python tool. The mean age of the delirium and non-delirium groups is presented as a 5-number summary (the mean±standard deviation; minimum age, 25th, 50th, and 75th percentiles; and maximum age; Fig. 2).
The probable factors were divided into 5 groups: unmodifiable, modifiable, preoperative, intraoperative, and postoperative factors. The unmodifiable factors consisted of age, sex, surgical history, drinking, height, and body mass index (BMI). The modifiable factors included a history of psychiatric drug or steroids use, smoking, diabetes mellitus, hypertension, cancer, and brain disease (Table 2). The preoperative and postoperative factors (Table 3) included blood analysis results for white blood cell (WBC) count, C-reactive protein (CRP), erythrocyte sedimentation rate (ESR), glutamic-oxaloacetic transaminase, glutamic-pyruvic transaminase, blood urea nitrogen (BUN) level, blood creatinine level, the estimated glomerular filtration rate (eGFR), blood sodium (Na) level, blood potassium (K) level, blood chloride (Cl) level, blood calcium (Ca) level, blood albumin level, fasting blood glucose level, hematocrit, and hemoglobin A1c. The intraoperative factors reviewed were the amount of inhaled and intravenous anesthetic agents, neuromuscular agents, volume of blood loss, operation time and the fluid volume used. In addition, the use of blood transfusion and the type of spine surgery (cervical or lumbar spine surgery) were included in the intraoperative factors (Table 3). All numerical values were calculated by the use of Python. The χ2 test was used to evaluate the differences in dichotomous variables. The Student’s t-test was used to evaluate the differences in normally distributed continuous variables. The Mann-Whitney U-test was used to evaluate the differences in the mean values between the groups for non-normally distributed variables.
Multivariate logistic regression models with backward elimination were constructed to identify the independent risk factors associated with the occurrence (positive or negative) of postoperative delirium. Factors with p<0.05 in the previous univariate analysis were included. Odds ratios and their 95% confidence intervals were calculated. A p-value of less than 0.05 was considered statistically significant.
RESULTS
1. Incidence and Characteristics of Delirium in All Patients
Postoperative delirium was found in 110 out of 3,581 patients (3.07%). The incidence of postoperative delirium increased with increasing age. The incidence was 1.53% in the <60-yearold group compared to 27.37% in the 85 to 89-year-old group (Table 1). The mean patient age was 66.0±13.7 years in the postoperative delirium group and 57±14.8 years in the non-delirium group (Fig. 2).
2. Risk Factors for Postoperative Delirium in the Age-matched Groups
There were 110 patients in the age-matched, postoperative delirium group and 228 in the age-matched non-delirium group. A univariate analysis was initially performed. Among the unmodifiable factors, height, and BMI, and among the modifiable factors, smoking history, a history of psychiatric medicine, and steroid use were statistically associated with postoperative delirium. There was no significant difference in sex, surgical history, or comorbidities (diabetes mellitus, hypertension, and cancer) (Table 2).
Among the preoperative factors, WBC count, CRP, ESR, BUN, eGFR, K, Cl, Ca, blood albumin level, and fasting blood glucose, and the postoperative factors, WBC count, ESR, CRP, eGFR, Na, Cl, and fasting blood glucose tended to be statistically associated with postoperative delirium. Regarding the intraoperative factors, intraoperative blood transfusions, the use of neuromuscular agents, and cervical spine surgery were statistically associated with postoperative delirium.
Multivariate stepwise regression analysis was conducted with factors found to be statistically associated with postoperative delirium in univariate analysis (Table 4). Smoking history (p= 0.008), the use of psychiatric medication (p=0.004), the use of steroids (p=0.041), preoperative CRP (p=0.001), blood Cl levels (p=0.006), fasting blood glucose levels (p=0.004), intraoperative transfusions (p=0.044), and postoperative CRP (p=0.040), ESR (p≤0.001), and blood Cl levels (p=0.005) were identified as significant risk factors for postoperative delirium.
DISCUSSION
Our study identified smoking history, the use of psychiatric medication, the use of steroids, preoperative CRP, Cl, fasting blood glucose, intraoperative transfusions, and postoperative CRP, ESR, and blood Cl levels as significant risk factors for postoperative delirium.
In previous studies, postoperative delirium was found in 10% to 60% of the patients who underwent surgery, with a particularly high incidence in orthopedic pelvic surgery and aortic surgery5,14,23,30). The mortality rate of hip fracture patients was higher in those who developed delirium than in those who did not15,18). For that reason, perioperative delirium is a great concern during the treatment of hip fractures. Generally, neurosurgeons have paid less attention to postoperative delirium after spine surgery due to the relatively low occurrence rates. A previous study14) speculated the reason because elective spinal surgeries are exposed to lesser stress than other emergency operations, such as femur neck fracture surgery. However, in the older population, the incidence of delirium after spine surgery is increasing highly and re-admission rate is increased in patients with postoperative delirium11). In the present study, the overall incidence is 3.07%, but the rate is increased by age to 27.37% in patients older than 85 years of the age.
Delirium is multifactorial and dependent upon a variety of risk factors22,27). Although the exact pathophysiology is unclear, various pathophysiological mechanisms have been suggested in different situations. Age is the most critically significant risk factor affecting postoperative delirium. It is widely accepted that postoperative delirium is more common in older patients 14,28). Brown et al.6) reported that approximately 25% of adults aged more than 65 years experienced delirium during hospitalization. Ushida et al.30) suggested that age-related decreases in melatonin levels could influence the circadian rhythm of patients. Another reason for the higher incidence of postoperative delirium among elderly patients may be a higher incidence of severe physical illness, chronic cerebral vascular disease, or medications for comorbidities14).
Smoking history was also identified as a significant risk factor for postoperative delirium. Cigarette smoking is believed to induce neuroadaptive changes in the brain, especially after cessation. These changes are related to an increase in the function of neurotransmitters that share a pathway with delirium. Microvascular changes in the brain caused by smoking might also lead to impaired cognitive function and reserve19). Another study suggested that nicotine withdrawal during hospitalization might cause postoperative delirium. For example, greater agitation was reported in a study of intensive care unit patients experiencing nicotine withdrawal12).
Changes in the level of neurotransmitters, such as decreased cholinergic activity, increased dopaminergic activity, and decreased gamma-aminobutyric acid-ergic activity, were also thought to be involved in the pathogenesis of delirium8,29). In our study, a history of using psychiatric medications, which changes the level of neurotransmitters and might induce delirium, was a statistically important risk factor for postoperative delirium7).
A history of steroid use was also reported to be a risk factor for postoperative delirium17,21). Although the pathophysiology of the effect of steroid on delirium is uncertain, a previous study suggested that a change in the circadian rhythm by steroids could be the cause. Ushida et al.30) suggested that the administration of high-dose steroids might influence circadian rhythm. Disturbances in circadian rhythm have been considered an important contributing factor to the development of postoperative delirium3,17,30).
Intraoperative blood transfusion was identified as a risk factor of postoperative delirium in this study. The pathophysiology of postoperative delirium associated with blood transfusions is unclear. However, an inflammatory response induced in the recipient could be the possible cause. Stored red blood cell units are known to contain activated inflammatory cells and inflammatory cytokines such as tumor necrosis factor-α, interleukin (IL)-6, IL-8, and IL-1824). These inflammatory mediators may involve transport across the blood-brain barrier and microglial activation, resulting in impairment. Cytokines may inhibit the synthesis and release of acetylcholine, leading to a central cholinergic deficit, a recognized cause of delirium4).
Although not identified as statistically significant risk factors in this study, other studies suggested that low hematocrit and hemoglobin levels were risk factors for postoperative delirium. Shi et al.23) suggested several hematogenous predictors of delirium after spinal surgery, including lower preoperative hematocrit and increased intraoperative blood loss. A low hematocrit might reduce the oxygen supply to the brain and lead to postoperative delirium14,25,30).
Pre- and postoperative CRP levels were identified as statistically important risk factors for postoperative delirium in this study. We think this might be related to the inflammatory response associated with delirium. Cerejeira et al.7) reported that the cerebral effect of systemic inflammation during the perioperative period may be aggravated by the anticholinergic effects of drugs administrated during this phase and be responsible for postoperative delirium16).
In the present study, abnormal postoperative Cl levels were related to postoperative delirium. Several previous studies showed that fluid and electrolyte imbalance was closely related to postoperative delirium10,31). An electrolyte disorder is a very plausible risk factor for postoperative delirium. A disturbance in Na or K levels is usually associated with body fluids disorders, including hypotonia or hyperosmotic dehydration31). However, the influence of different electrolytes on postoperative delirium remains controversial10).
This study had a few limitations. Firstly, it was a retrospective cohort study, and an insufficient number of risk factors were analyzed. Due to the multifactorial nature in development of delirium, other potential risk factors not included may influence and interact the occurrence of the postoperative delirium. And there might be many potential factors that we did not consider. Secondly, patients with postoperative delirium were diagnosed and treated by the psychiatric department after consultation. Hence, patients with mild symptoms of delirium did not receive treatment and could have been excluded.
CONCLUSION
Postoperative delirium was found in 3.07% of the patients after elective spine surgery at a single center. Smoking history; the use of psychiatric medication; the use of steroids; preoperative CRP, Cl, and fasting blood glucose levels; intraoperative transfusion; and postoperative CRP, ESR, and blood Cl levels were identified as significant risk factors for postoperative delirium. Dedicated perioperative care should be performed to prevent postoperative delirium in patients with the above risk factors.