INTRODUCTION
Venous malformations (VMs) are a commonly encountered entity in clinical practice, with an estimated incidence of 1 to 2 in 10,000 births and a prevalence of 1%4,19). VMs are composed of abnormal collections of veins with a variable luminal size and wall thickness, often multiple17). They are often less well-circumscribed than are vascular tumors, such as infantile hemangiomas, and can be interspersed with adipose tissue or within various kinds of atrophic or degenerative muscle13). Although all VMs are present at birth, but they are also identified in adolescence and adulthood13). VMs occur at a frequency of 40% in the head and neck region, 40% in the extremities, and 20% in the trunk2). VMs in the extremities often violate surrounding fascial planes and can infiltrate subcutaneous tissue, muscle, bone, joints, neurovascular structures, and even viscera2).
Intramuscular VMs comprise an uncommon subgroup of VMs15). They are often mistaken for tumors, because of a similar presentation and because of improper nomenclature8). Although most intramuscular VMs in the extremities have been reported to present with a growing palpable mass with or without pain10), the development of neurological symptoms is rare. The authors report a rare intramuscular VM originating from the brachialis muscle and showing symptoms of median nerve involvement.
CASE REPORT
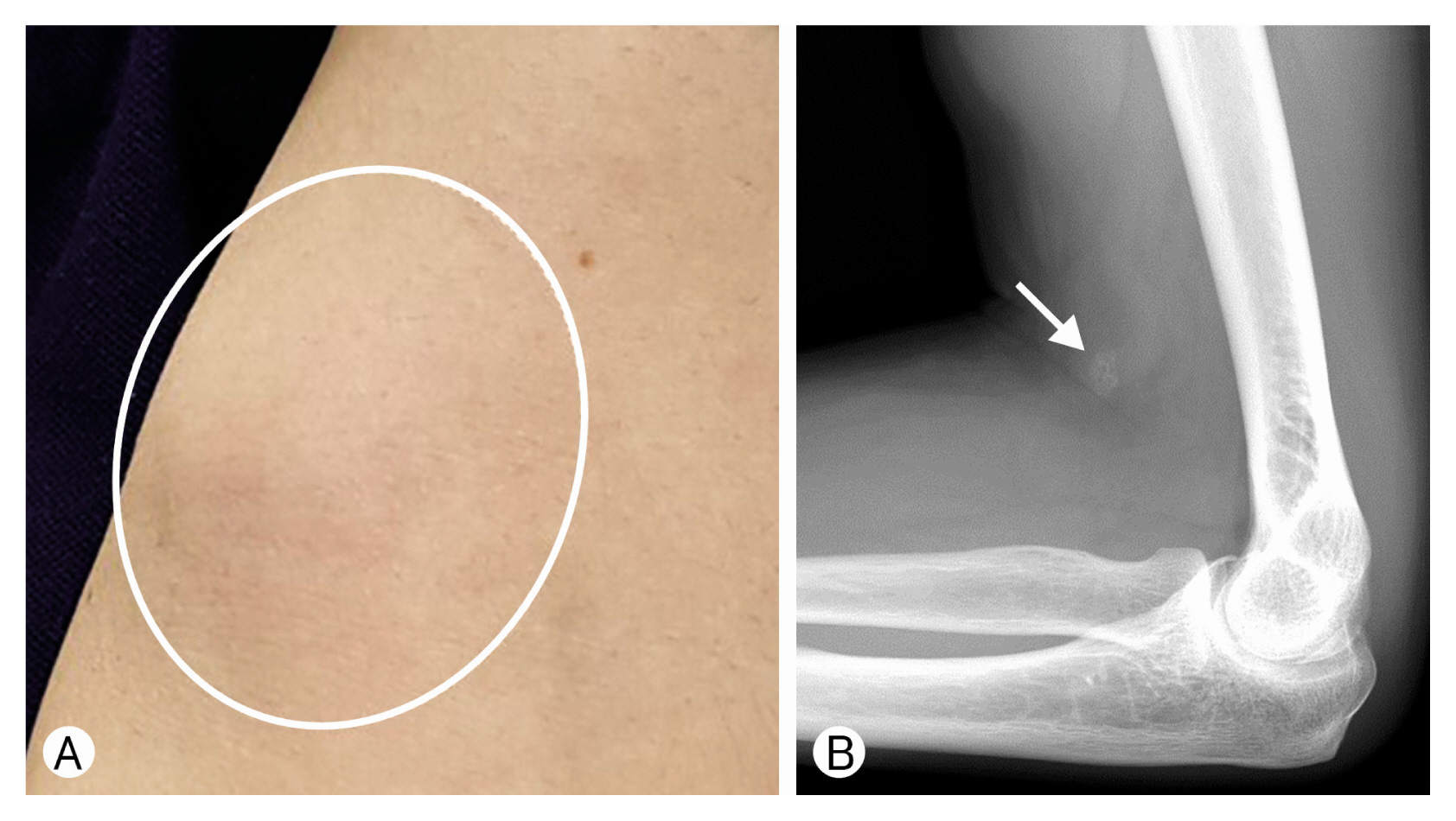
A 58-year-old, right-handed male patient presented with a gradually growing mass in the distal upper arm and mild weakness in left-hand grasping. The mass occurred 6 months prior to the presentation, and there was no pain when it first occurred. The mass gradually increased; in the morning, it became larger, and in the afternoon, it became smaller (Fig. 1A). A month previously, when he touched the mass, he felt tenderness and tingling in the thenar area of his left hand. Two weeks later, the mass got bigger, and his left-hand grip weakened; when he grabbed an object, he began to drop it.
On examination, there was no objective weakness in forearm pronation, wrist flexion, flexion of the first 3 digits and thumb opposition, or abduction, which are innervated by the left median nerve, nor any objective sensory disturbance in the radial 2/3 of the palm that is innervated by the palmar cutaneous branch of the median nerve. There was no tenderness in the mass itself, but when the medial of the mass was pressed, there was pain along with tingling instantaneously in the thenar side of the left palm. It was not mobile. X-ray examination showed a small calcification in the soft tissue in front of the distal humerus (Fig. 1B). Magnetic resonance imaging (MRI) of the upper extremity revealed a 3-cm-sized, lobulated mass within the brachial muscle in the distal upper arm (Fig. 2B). A T2-weighted fast spin-echo image revealed a well-demarcated, lobulated mass with a hyperintense signal (Fig. 2B). Inside the hyperintense lesion, the heterogeneous appearance with low signal intensities indicated hemorrhage or thrombosis, and often dilated vascular structures were identified. In the T1-weighted image, it was isointense with lesion extent appearing inconspicuous to adjacent muscular tissue (Fig. 2C). Gadolinium administration resulted in heterogeneous enhancement within the mass (Fig. 2C). The veins of the antecubital fossa were dilated and showed ectasia. The left median nerve was not directly involved by the lesion, but was displaced by the swollen brachialis muscle (Fig. 2D). With these unique MR findings, the lesion was thought to be a low-flow, VM. Considering the gradual enlargement of the mass and worsening of the pain and neurological symptoms, surgery was planned, and consent was obtained.
After we made a lazy S-shaped vertical incision along the medial antecubital area, we carried dissection down to the antebrachial fascia. After securing the left median nerve, we dissected the swollen brachial muscle under microscopic vision. We did circumferential dissection by identifying a fairly firm venous structure (Fig. 3A). Between the muscle fibers, multiple dilated large venous channels and fibrous septa were identified and ligated with hemoclips. Bleeding venous structures and dilated drainers were controlled by bipolar coagulation. The VM was firmly attached to the surrounding brachialis muscle. However, no difficulty was found in complete excision (Fig. 3B, C). No neurological abnormalities were observed after complete excision, and the mass did not appear again. By one year after surgery, the mass was no longer present, and there was no abnormality in the left hand and arm movements and sensations.
DISCUSSION
1. Intramuscular VM
Identification and classification of vascular anomalies were hampered historically by the use of confusing nomenclature7). Early classification suggested by Virchow20) and Wegener21) classified vascular lesions according to the pathologic appearance of the vessel7). Vascular growths were divided into angiomas and lymphangiomas without consideration of the biologic behavior and natural history of the vascular lesions7). Consequently, there was a tendency to identify any vascular anomaly as a hemangioma5-7,13,16). A variety of terms including “venous angioma”, “cavernous angioma”, “cavernous hemangioma”, and “phlebangioma” have been used in the medical literature to describe these anomalies5,7). These terms have led to confusion with the more common proliferating or true hemangiomas of infancy5,7). For example, capillary hemangioma, nevus flammeus, and port-wine stain have all been used in the literature to describe a capillary malformation of the skin16).
In 1982, Mulliken and Glowacki16) proposed a modern classification of vascular anomalies according to the lesion’s biologic and pathologic differences; all vascular anomalies were assigned to 1 of 2 broad categories: hemangiomas and vascular malformations. The former category was later expanded to include vascular tumors. The suffix “-oma” was to be reserved for only those lesions exhibiting increased cellular turnover, the classic example within this category being the infantile hemangioma5,13). The term “vascular malformation” was applied to those lesions present at birth growing commen-surately or pari passu with the child13). The vascular malformations were composed of normal “mature” flat endothelial-lined vascular spaces with a normal rate of cell turnover and were further subdivided into capillary malformations, VMs, arterial (arterio venous) malformations, and lymphatic malformations5,13). In 1993, Jackson et al.9) classified vascular malformations according to flow patterns instead of the former anatomicopathological classification for ease of investigation and treatment (Table 1). They simplified flow patterns within vascular malformations as either low-flow (VMs) or high-flow (arteriovenous malformations), keeping separate categories for lymphangiomas and hemangiomas, with the purpose of creating “system directly related to investigation and treatment”9).
2. Clinical Manifestation and Diagnosis
The diagnosis of VM and differentiation from other vascular malformations can be usually made by clinical history and physical examination13). Because VMs are congenital lesions, they may be identified at birth. However, they are usually identified from infancy to puberty, which is the period of greatest enlargement of the lesion7). Continued linear growth within the malformation despite the end of somatic growth in late adolescence often results in clinical manifestations later in life and is typically the case in deeper lesions20).
VMs typically appear as soft, compressible, blue-tinged masses that can enlarge with dependent position and Valsalva maneuver1). The blue tinge is considered pathognomonic and is caused by dilated venous channels within the dermis6). Forty percent of VMs occur in the head and neck region, and may involve the mucosa of the tongue, palate, orbital, mandibular, or neck region, even direct involvement of the ophthalmic branch of the trigeminal nerve in the face2,11). VMs in the extremities often infiltrate the surrounding tissues13). As such, patients commonly experience symptoms as a result of several mechanisms. Venous engorgement secondary to dependent positioning, exercise, after prolonged stasis, or after morning awakening frequently results in significant swelling and pain13). Mass effect may cause local compression of the nerve and muscular contracture or restricted range of motion of an adjacent joint13). Local hemorrhage and local stasis on a background of chronic low-grade intravascular coagulopathy thromboembolic state within the lesion can occur13,14). In the current case, a VM occurred in late adulthood at the age of 58 and originated from the brachialis muscle. It showed swelling in the morning due to venous stasis and symptoms of left median nerve irritation due to local mass effect.
MRI is the imaging modality of choice for VMs13), which classically appear as either isointense or hypointense on the T1-weighted sequences12,13). The lesions appear focal, diffuse, or demonstrate lobulated margins. A more heterogeneous appearance can be identified in the setting of hemorrhage or thrombosis, and often dilated and serpiginous vascular structures can be identified compatible with abnormal veins13). Lower signal area or signal voids may represent dystrophic calcification or phlebolith on all imaging sequences12). In addition to calcification, lower signal areas on T2 can be caused by either vascular channels or fibrofatty septa12). Gadolinium administration results in homogeneous or heterogeneous enhancement within the substrate of a VM13).
3. Treatment of Intramuscular VM
Treatment is generally indicated if the lesion causes pain, functional impairment, or aesthetic problems, as in craniofacial lesions2). With the exception of some superficial VMs where laser therapy is effective, VMs are generally treated with direct surgery and sclerotherapy13). Surgical resection is considered preferable if the lesion could be completely removed so as to avoid recurrence8). This includes patients with focal well-defined VMs that are thrombosed, confined to a single or specialized muscle group, or causing a neurological or compression syndrome, and patients where there is a good possibility of anatomical and functional restoration8). Many lesions are infiltrative, however, and involve multiple muscle groups or fascial planes where surgical resection results in an unacceptably high functional and cosmetical deficit18). Sclerotherapy has been increasingly incorporated in surgical regimens and now has been considered as an adjunct to surgery or the stand-alone therapy of choice for most VMs3,13,18). We chose surgical resection in the current case because the lesion was well localized within the brachialis muscle and caused local neurological symptoms by mass effect. The treatment resulted in complete relief of the symptoms of VM, with no recurrence up to 2 years after surgery.
CONCLUSION
Here, we report on a rare intramuscular VM originating from the brachialis muscle in the left arm, which caused the local mass effect, showing the symptoms associated with irritation of the median nerve. The lesion was diagnosed through a typical MR imaging finding. Because the lesion was well-localized within the brachialis muscle, surgical resection resulted in complete symptomatic relief without recurrence.