INTRODUCTION
Chondromas are benign tumors arising from cartilaginous structures and are susceptible to metaplasia and malignant degeneration 8). Most chondromas are occurring in the fingers, followed by the hands, toes, and feet. Chondromas originating in the spine are very rare.
The common site of the spine is not clear. But, the previously reported cases of spinal chondromas in cervical and lumbar lesions are more than 15 cases. Relatively, only 1 case is reported in the thoracic spine6). Most spinal chondromas remain asymptomatic. But, few patients have paravertebral swelling and pain, and some complain of radicular pain and neurologic deficits.
We report a rare case of an extradural lumbar spinal chondroma located in the foraminal zone resulting in radicular pain.
CASE REPORT
A 74-year-old woman presented at our department complaining of back pain and right lower extremity pain and numbness for 1 year. She underwent lumbar surgery at the L4-5 level at another hospital.
On neurologic examination, motor weakness, muscle atrophy, and pathologic reflex were not noted.
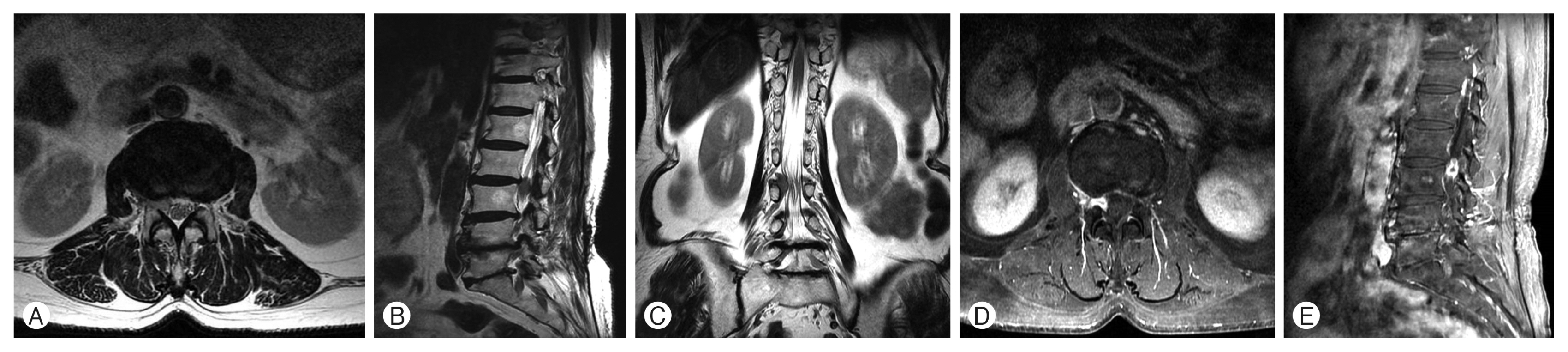
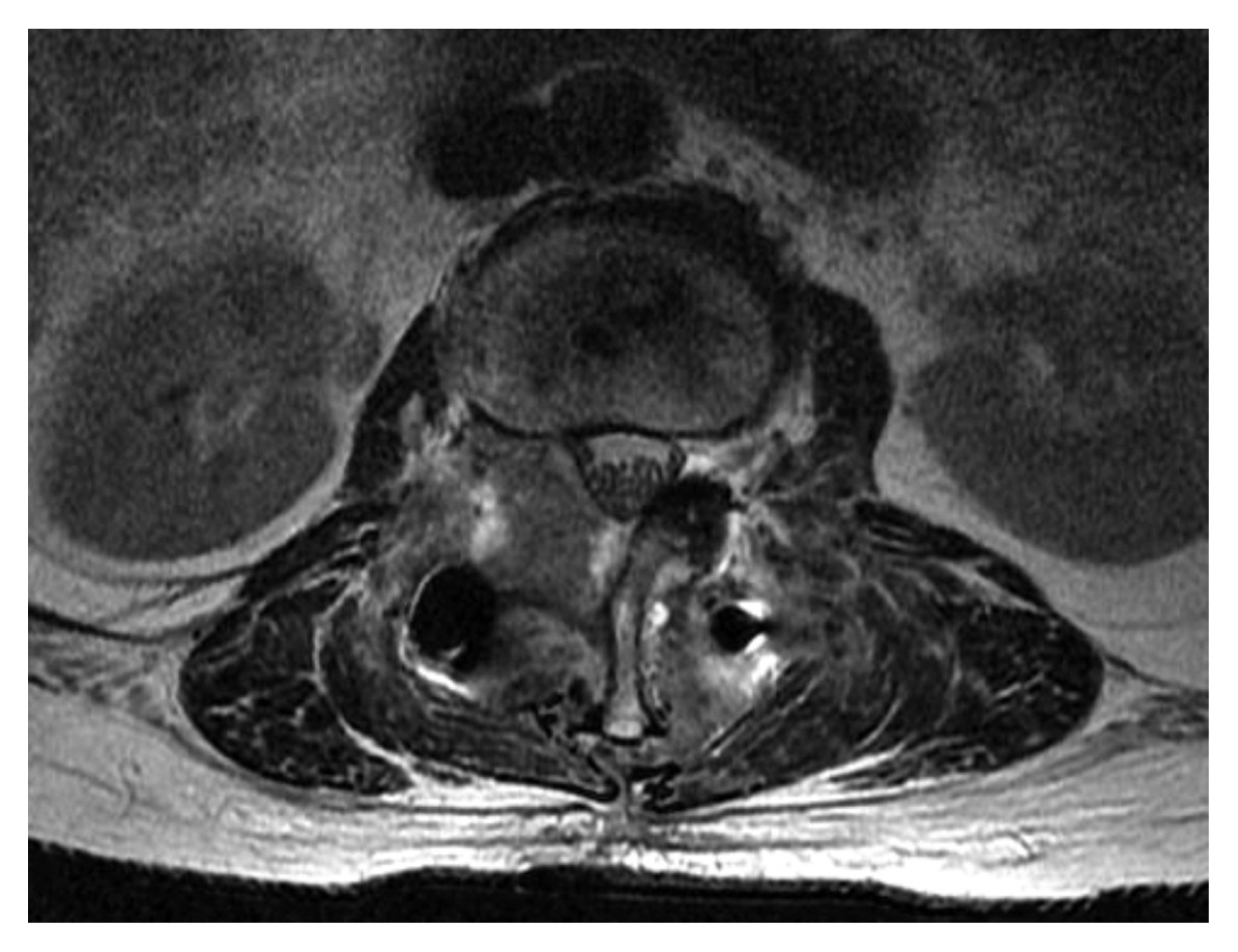
Magnetic resonance imaging (MRI) demonstrated an oval-shaped mass-like lesion in the epidural space at the right foraminal zone on L2-3. The mass had an isointense signal on T1- and T2-weighted images (WIs). The mass showed strong peripheral rim-like enhancement and central non-enhancing foci (Fig. 1).
She underwent surgery. After hemilaminectomy and facetectomy, total tumor removal was performed. We conducted transpedicular screw fixation for the prevention of postoperative spinal instability. Decompression of the dura mater was observed intraoperatively. The mass was pinkish, soft, friable, and well-dissected from the dura (Fig. 2).
After surgical treatment, back pain and radiating pain were relieved. Histopathological examination confirmed the mass to be a chondroma (Fig. 3).
On a follow-up MRI examination, total mass removal was verified (Fig. 4). The patient was discharged without complications.
DISCUSSION
Tumors originating from the cartilage are classified as chondromas, osteochondromas, chondroblastomas, and chondromyxoid fibromas. Chondromas are subdivided into 2 types: enchondroma and periosteal chondroma7). When chondromas are found distant from the bones, they are referred to as soft tissue chondromas11). Enchondromas tend to grow as expansile patterns, and periosteal chondromas are exophytic9). Spinal chondromas may be derived from hyperplasia of immature spinal cartilage from metaplasia of the connective tissue in contact with the spine or annulus fibrosus8).
Chondromas in the spine constitute about 3% and 4% of all chondromas4,7,9). Cartilage-forming tumors account for 2% of all spinal tumors3). Chondromas are involved in the vertebral structure, vertebral body, neural arch, and spinous and transverse processes. The neural arch is the most common site of lumbar spine chondromas7). A rare spinal intradural chondroma has also been reported4).
Most cervical spine chondromas occur in young male adults, and the initial symptoms are motor weakness and sensory change1). Neurologic symptoms are more common in adults aged <40 years5). Symptomatic chondromas on the lumbar spine are rare and can result in back pain, numbness, and hypoesthesia of lower extremities2), but radicular symptoms are not common3). A large number of chondromas on the lumbar spine are asymptomatic because of their slow-growing nature. When those are not involving the spinal canal, most of the cases are also asymptomatic.
A differential diagnosis between benign chondroma and well-differentiated chondrosarcoma is difficult, but important2). Chondromas are usually isolated as single lesions and can undergo malignant transformation. When multiple chondromas are noted, Ollier disease and Maffucci syndrome should be considered. Multiple chondromas can undergo more sarcomatous changes than a single lesion9).
Plain radiography may show only smooth erosion of the bony structure, which could have been in direct contact with tumors or may also show a well-circumscribed lytic lesion with a widened neural foramen. Computed tomography (CT) and MRI are important tools for evaluating tumor growth, invasion, and the relation of adjacent structures3). CT can be used to demonstrate hyperdense calcified lesion9,12), and is the preferred modality to demonstrate osseous structures of tumors. Furthermore, extraosseous soft-tissue edema close to the mass can be detected on T2-WIs5). The relatively small size and absence of soft tissue invasion suggest a benign chondroma rather than a malignant nature6). Chondromas usually present as an isointense signal on T1-WIs and hypointense to isointense signals on T2-WIs, but the signals can be variable. Peripheral rim enhancement has been observed on gadolinium-enhanced MRI scans7,10,12).
Chemotherapy is ineffective, and radiotherapy is unnecessary if total tumor removal is performed. Radiotherapy is considered when the tumor is not completely removed1).
Asymptomatic chondromas in the spinal canal are more common than symptomatic chondromas in the spine. We report a rare case of lumbar spinal chondroma accompanied by radicular symptoms.