INTRODUCTION
A schwannoma is a benign, encapsulated peripheral nerve sheath tumor. An intramuscular schwannoma is extremely rare and grows slowly. The symptoms of an intramuscular schwannoma are dependent upon the site of origin. In most cases, the symptoms are ambiguous, making a preoperative diagnosis difficult. Further, specific motor weakness due to motor branch involvement is uncommon10). We report a rare case of schwannoma in the dorsal paraspinal muscles.
CASE REPORT
A 79-year-old man was admitted to the hospital because of tenderness on the right side of his back. A palpable mass was identified 6 years prior to his admittance. No neurological deficits were detected, and the laboratory data were within normal limits; the patients’ medical history was unremarkable.
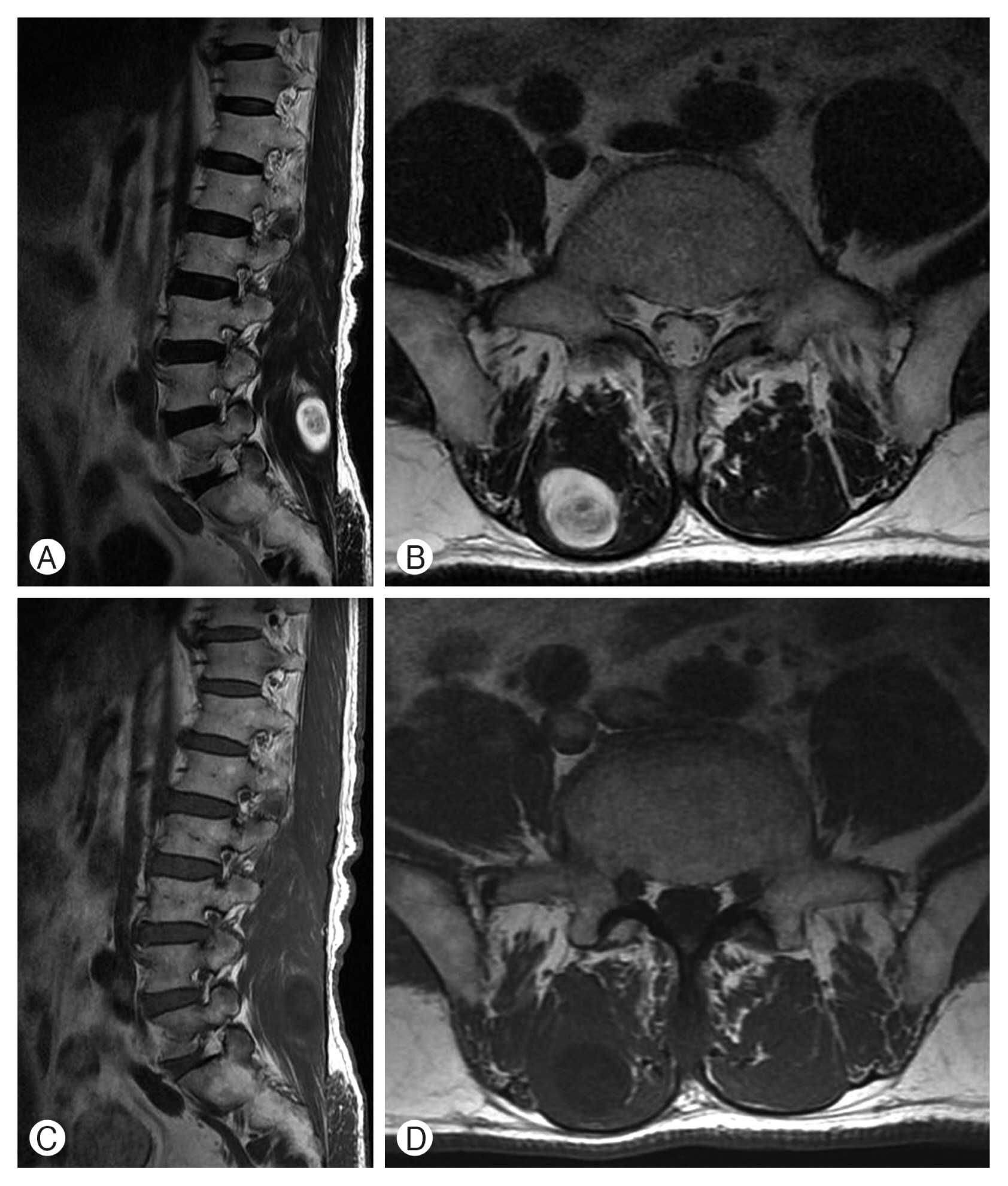
The mass was observed in the right multifidus muscles at the L5 level using magnetic resonance imaging (MRI). The MRI scan showed an oval-shaped tumor measuring 2.0×2.0×3.5 cm. There was a well-defined and heterogeneous intermediate signal on the axial T1-weighted image (WI), and a strong enhancement of central mass lesion was noted (Fig. 1). The preoperative diagnostic evaluation suggested that the growth was a metastatic, sarcoma, or a peripheral nerve sheath tumor.
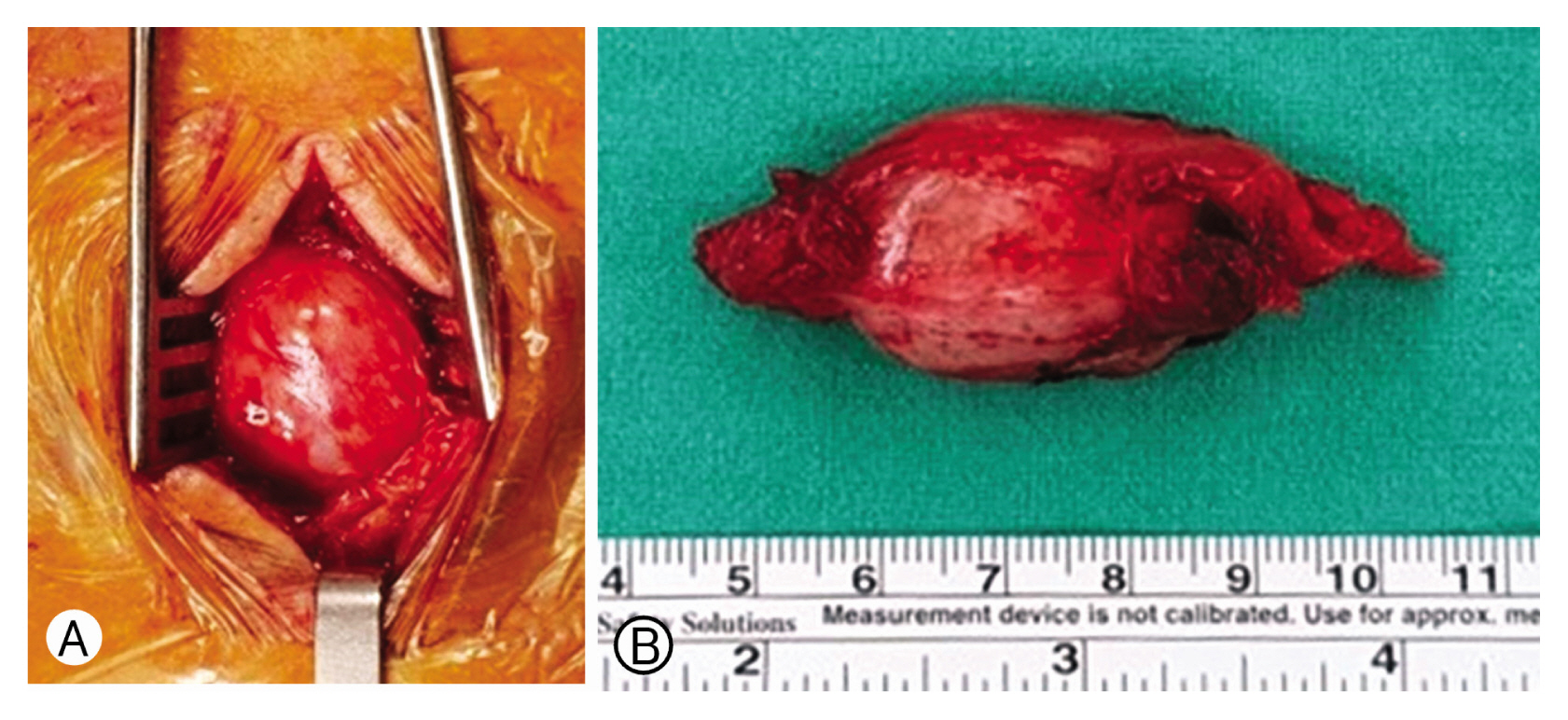
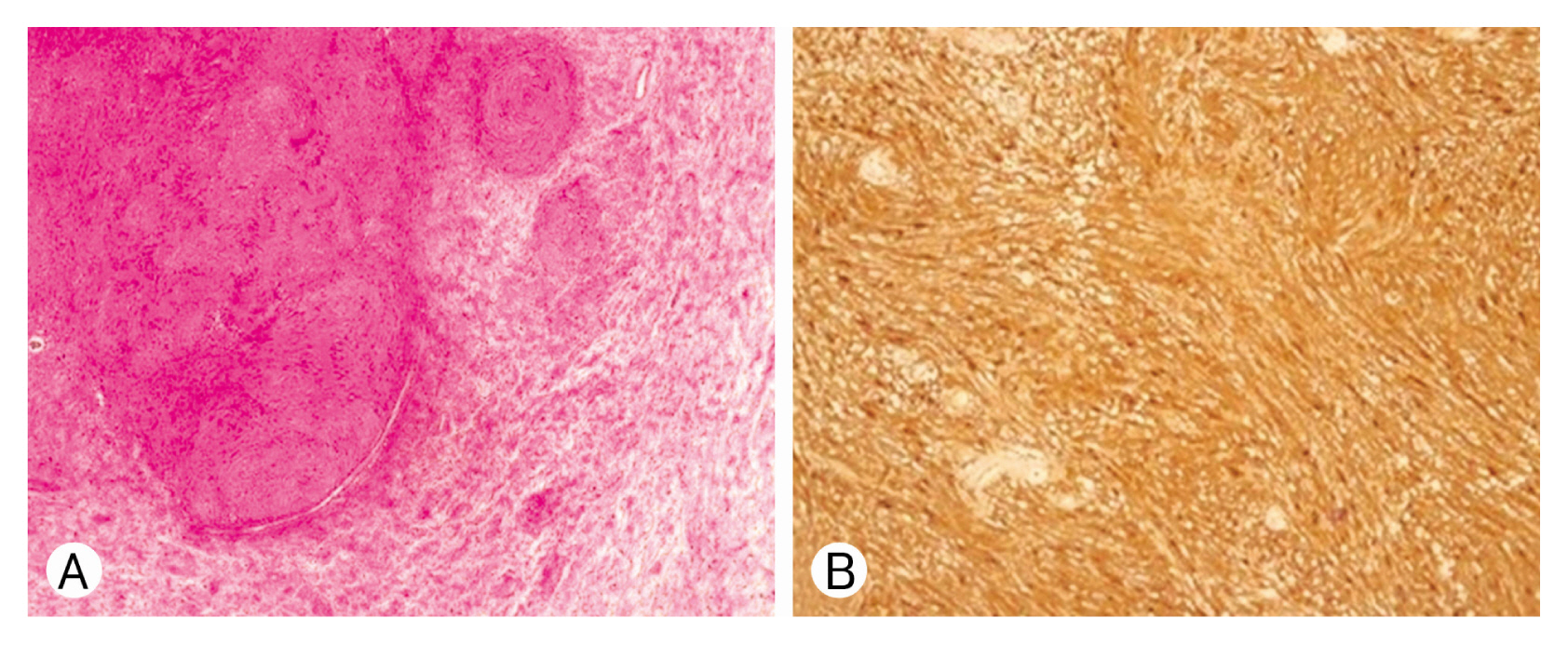
The patient underwent surgery, and the mass was completely excised. The mass was pinkish and well encapsulated with clear margins in the multifidus muscles and could be distinguished from the surrounding structures (Fig. 2). Microscopically, the tumor was composed of compact spindle cells (Antoni A) alternating with loosely arranged foci (Antoni B) (Fig. 3A). Immunohistochemistry showed diffuse, high S-100 protein expression, and S-100 immunohistochemistry was positive (Fig. 3B). Histopathological analysis identified the mass as a schwannoma.
There were no immediate neurological deficits following surgery, and the patient was discharged with decreased tenderness.
DISCUSSION
The most common benign soft-tissue masses are lipomas and their variants. Moreover, fibrous histiocytoma, nodular fasciitis, hemangioma, and schwannoma may occur in soft tissues, in this order of frequency4,11).
Schwannomas are benign tumors that arise from nerve sheath cells of peripheral nerves but rarely from within the muscle tissue. Less than 1% become malignant and transform into a form of cancer known as neurofibrosacroma11). Progressive rapid growth with pain and cystic changes may be signs of malignant transformation2). Although schwannomas can occur anywhere in the body, typical schwannoma cases are observed in the head and neck, with rates of 25% and 45%, respectively 11). About 3-quarters of benign solitary schwannomas are located in the upper limb arising from the brachial plexus or other nerves within the posterior triangle of the neck5). Complete surgical resection is the treatment of choice anywhere within the spinal axis6).
Intramuscular schwannomas originate from a small nerve branch within the muscle, and they are uncommonly associated with neurological symptoms including radiating pain, numbness, or motor weakness8). In cases of the psoas muscle involving schwannoma, abdominal pain and femoral nerve neuropathy may occur1,3,7). In our case, intramuscular schwannoma occurred in the multifidus muscle at the L5 level. Our patient complained of tenderness without radiating pain and lower extremity weakness.
The dominant nerve of the paraspinal muscles is the lumbar dorsal ramus nerve, a branch of the spinal nerve that forms from the dorsal root. The dorsal ramus nerve innervates a narrow strip of the skin and muscle along the back. This distribution of the nerve is of prime importance for the diagnosis of a nerve sheath tumor4,11).
In MRIs’, the lesion may have intermediate signal intensity on T1-WI, and heterogeneous on T2-WI2). After contrast enhancement, the cystic lesion and well-enhanced peripheral or solid mass lesions are clearly distinct from each other. In the split fat sign, entering and exiting nerve in low-signal, and a thin hyperintense rim were detected10). Low signal margin and fascicular sign on MRI are strong suggestive findings for diagnosing schwannoma10). The target sign was observed on T2-WI. This sign corresponded to the Antoni A area centrally and hyperintense peripheral rim similar to the Antoni B area. The MRI remains an important diagnostic tool; diffusion-weighted MRI may be used to differentiate benign paraspinal schwannomas from those of malignant nature9). The typical signs of schwannomas are more common in major nerve schwannomas than intramuscular schwannomas12).
The Antoni A area is composed of compact spindle cells arranged in short bundles or interlacing fascicles. The Antoni B area is highly vascularized, less cellular, and lacks distinctive architectural structures1). Immunohistochemically, strong S-100 protein expression was observed.
There was possibly only one case of dorsal ramus nerve schwannoma within the erector spinae muscles4). This case report describes a rare paraspinal schwannoma located in the multifidus muscle.