INTRODUCTION
Eosinophilic granuloma (EG), the mildest form of Langerhans cell histiocytosis (LCH), is a benign and unifocal bone lesion. Pathologic characteristics of EG are lysis of normal bony tissue with proliferation of bone-marrow-derived antigen-presenting cells3). EG mostly occurs in children, adolescents, and young adults, and the most commonly involved site is the skull8). The presenting symptom and prognosis of EG are usually benign; however, the spectrum of clinical course varies from spontaneous regression to relapse, and the etiology is also heterogeneous 3). Herein, we report a case of EG after minor head trauma in a pediatric patient treated with surgical excision successfully.
CASE REPORT
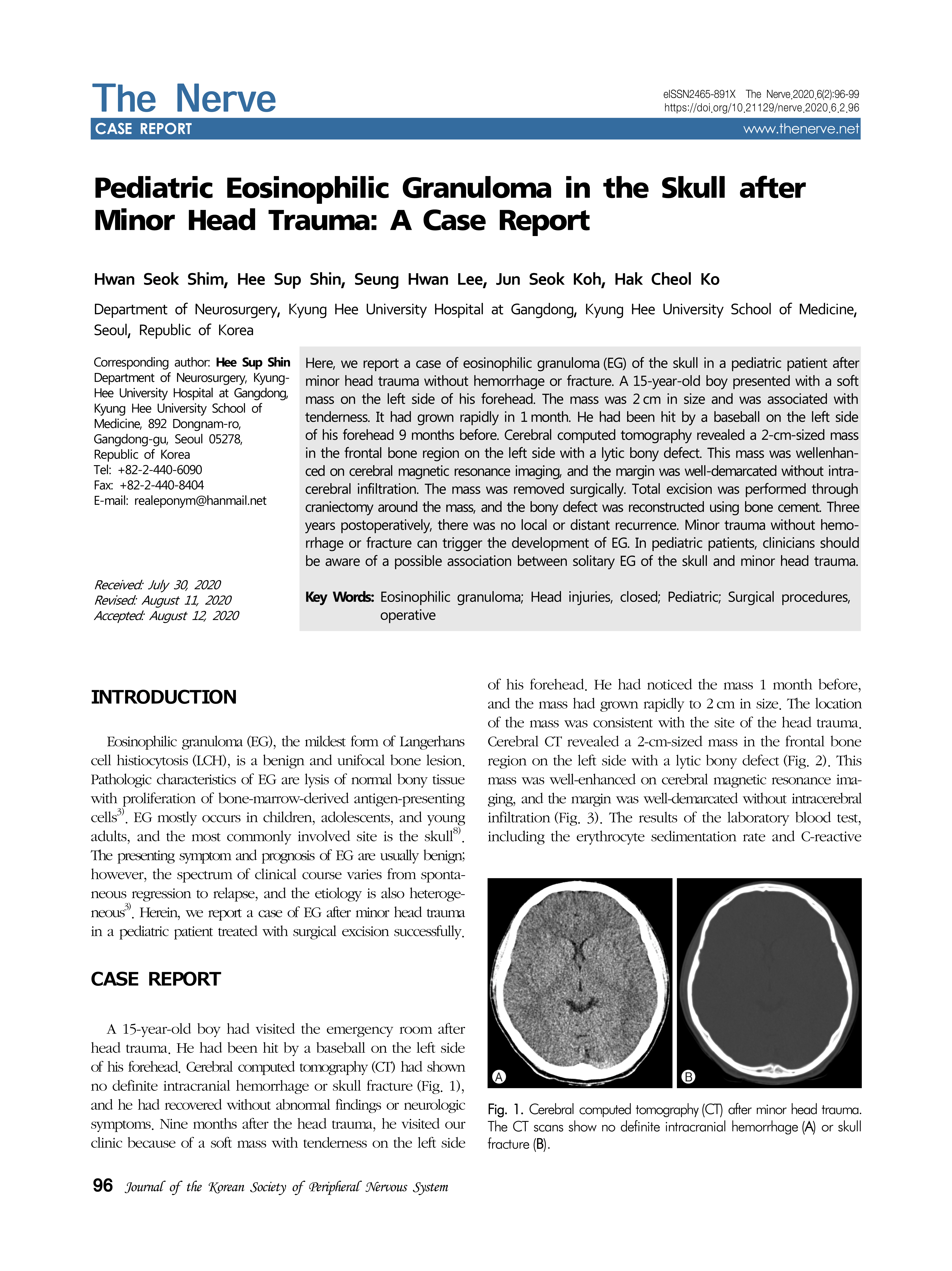
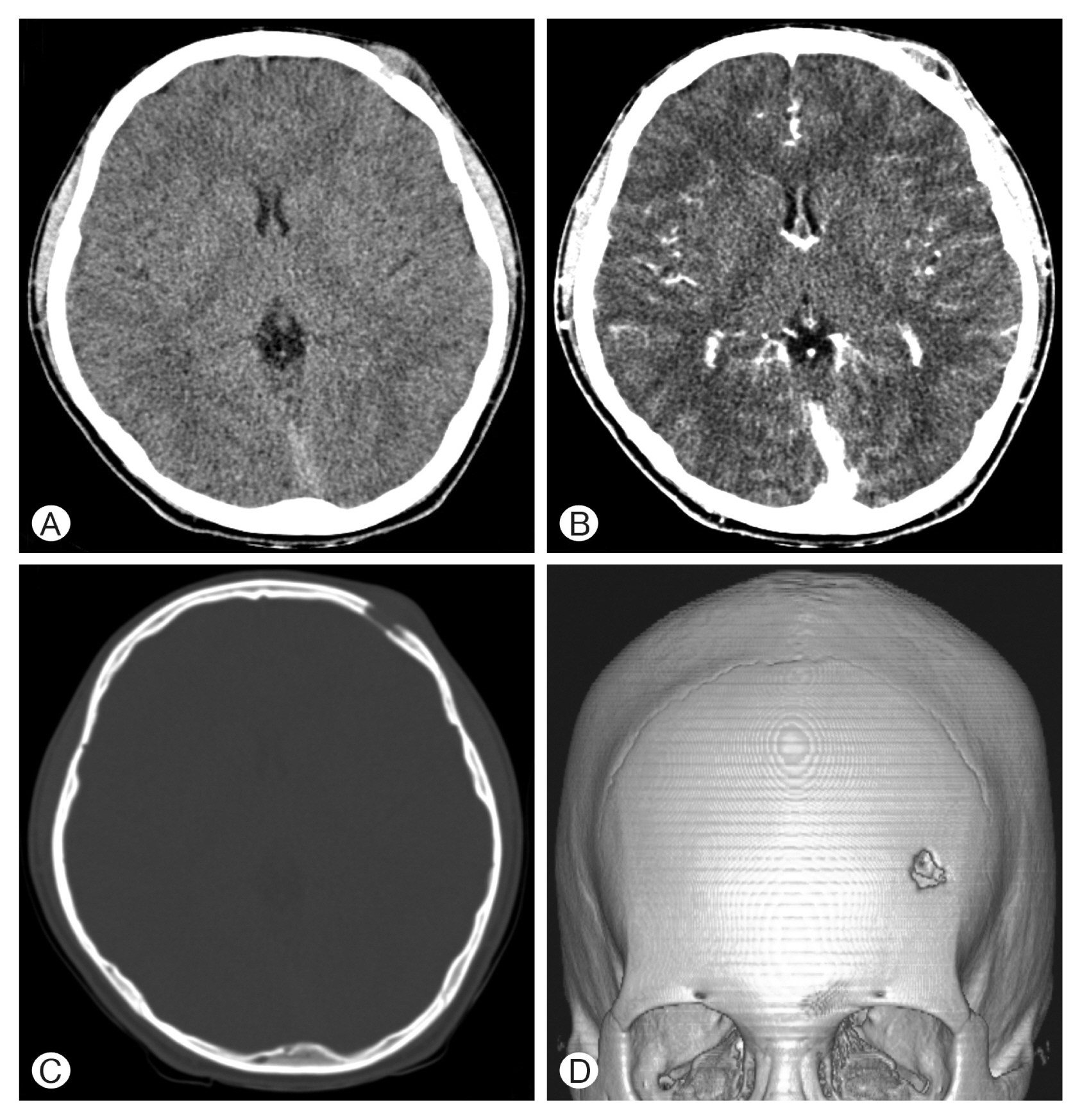
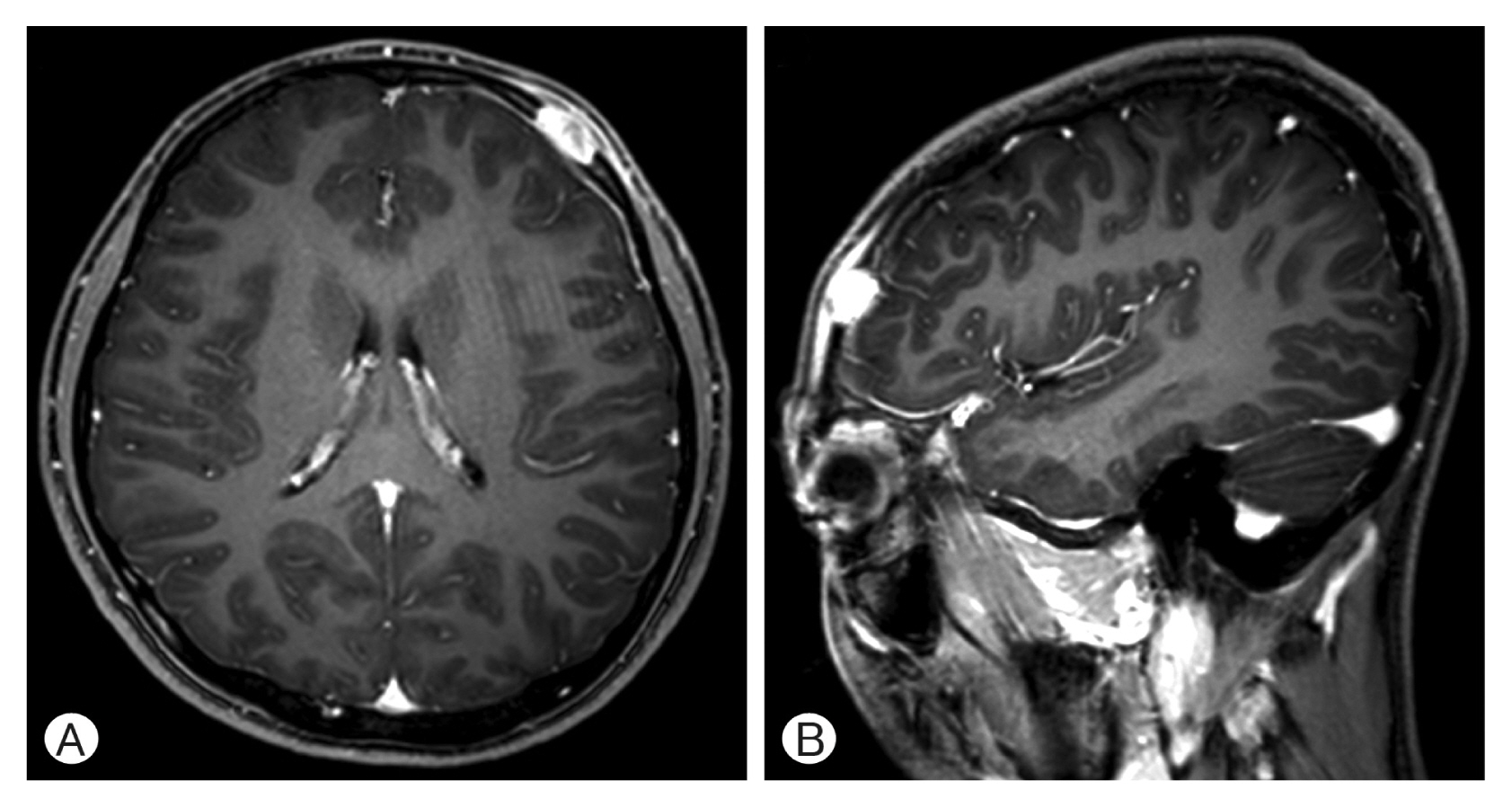
A 15-year-old boy had visited the emergency room after head trauma. He had been hit by a baseball on the left side of his forehead. Cerebral computed tomography (CT) had shown no definite intracranial hemorrhage or skull fracture (Fig. 1), and he had recovered without abnormal findings or neurologic symptoms. Nine months after the head trauma, he visited our clinic because of a soft mass with tenderness on the left side of his forehead. He had noticed the mass 1 month before, and the mass had grown rapidly to 2 cm in size. The location of the mass was consistent with the site of the head trauma. Cerebral CT revealed a 2-cm-sized mass in the frontal bone region on the left side with a lytic bony defect (Fig. 2). This mass was well-enhanced on cerebral magnetic resonance imaging, and the margin was well-demarcated without intracerebral infiltration (Fig. 3). The results of the laboratory blood test, including the erythrocyte sedimentation rate and C-reactive protein, were normal, except for mild eosinophilia. Because the patient complained of tenderness and rapid growth of the mass, we decided to perform surgery for excision of the mass.
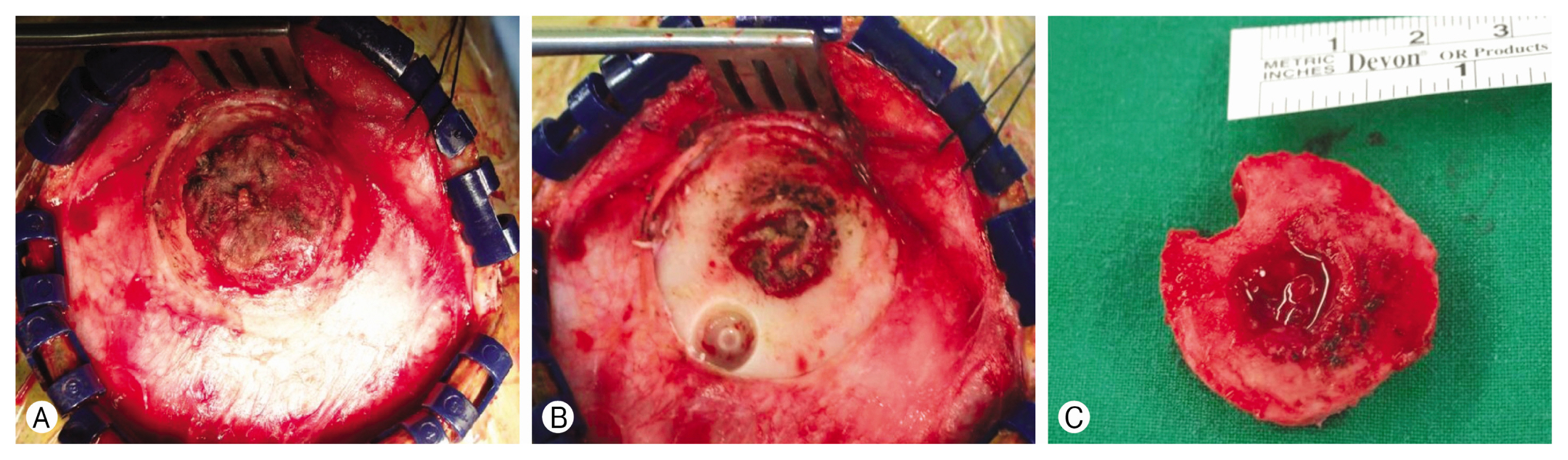
The patient was operated under general anesthesia. The galeal layer was dissected carefully following skin incision at the hairline. After reflection of the scalp flap, a reddish mass was exposed (Fig. 4A). The mass protruded to the extracranial space from the base of the lytic bony space. We excised the protruded mass first (Fig. 4B) and then removed the base of the mass with a bony flap around the mass (Fig. 4C). We confirmed that the dura mater was intact without any tumor invasion. The tumor was removed successfully, and the bony defect was reconstructed using bone cement. Postoperative cerebral CT showed complete removal of the mass (Fig. 5), and the patient recovered without procedure-related complications.
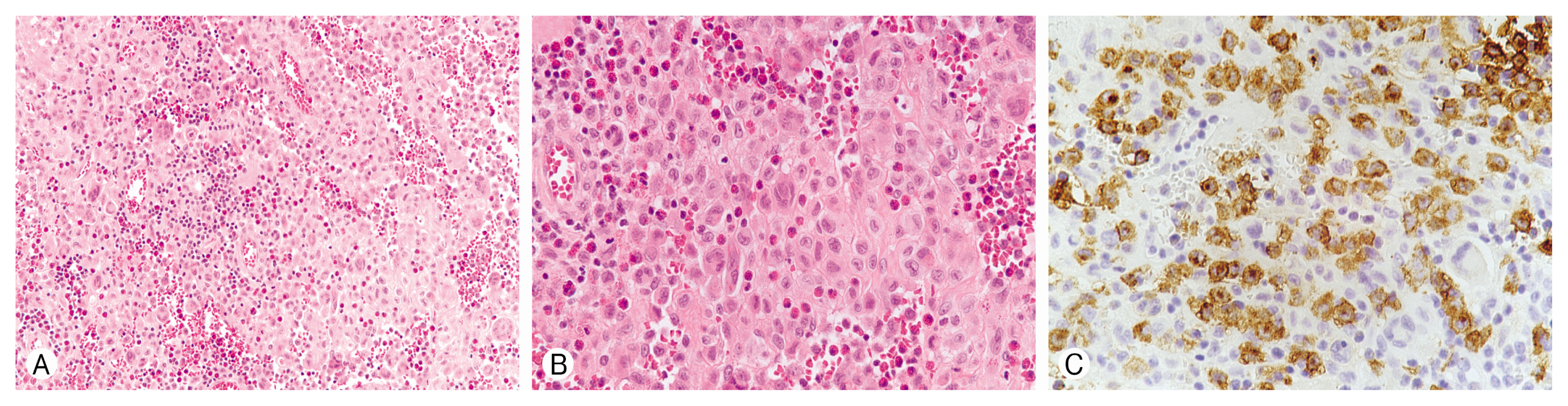
Histopathology showed clusters of oval Langerhans’ cells and a large number of eosinophils and osteoclast-like giant cells (Fig. 6A, B). In immunohistochemical staining, the majority of cells showed immunoreactivity for CD1a (Fig. 6C). These findings were consistent with LCH. We referred the patient to a pediatrician for the work-up of LCH. He underwent chest and abdomen CT, positron emission tomography/CT, and bone scintigraphy. The results of imaging studies were unremarkable. During a follow-up period of 3 years, the patient had no neurologic abnormalities. Cerebral CT performed 2 years postoperatively showed no recurrence.
DISCUSSION
LCH is a rare disease entity of the unifocal or multifocal disorder of the bone or soft tissue. Its incidence in childhood is regarded as 5.4 to 8.9 cases per million children per year10). This disease may occur in any age group, but children and young adults are most often affected. The clinical presentation varies in organ involvement as skin only, monostotic, polyostotic, multi-system, and organ dysfunction3). Among all types of LCH, EG is the mildest form8), which constitutes 70% of all LCH cases4). EG can involve multiple bony lesions; however, single lesions are more common. The most frequently affected site is the skull of the lytic lesion, followed by the mandible, spine, ribs, and long bones2,18). In cases of skull lesions, the most common symptom is a gradually growing mass with tenderness, particularly in the frontal and parietal bone regions. The typical radiologic findings are punched-out, sharply defined, lytic lesions of the skull. Histologically, infiltration of Langerhans’ cells, presence of eosinophilic and neutrophilic granulocytes, and granuloma formation are diagnostic. The clinical course is usually benign, and spontaneous regression may occur5,17).
Although the exact etiology of EG is not fully understood, an abnormal inflammatory reaction, autoimmune disease, and excessive proliferation of Langerhans’ cell are regarded as possible etiologic factors. Head trauma can also be considered as an etiologic factor. Some large case series documented that 33% to 50% of solitary skull EG patients had a history of head trauma1,6,19), and minor head trauma without definite hemorrhage or skull fracture could also result in solitary EG9). The interval from the trauma to the diagnosis is relatively short and ranges from 1 week to a few weeks9,11,12,14). In the present case, the patient had minor head trauma without hemorrhage or fracture before EG development, and the time interval of 9 months between the trauma and the diagnosis was quite long compared to previous reports. It is uncertain whether head trauma plays a key role in EG occurrence; however, it can be a possible mechanism for EG occurrence that triggers the amplification of abnormal inflammatory reactions at the local trauma site9).
Surgical excision is recommended for the treatment of solitary EG of the skull. The total excision through craniectomy around the mass is the most common form of surgical excision. In some cases, curettage of the lesion can be considered. Radiotherapy or chemotherapy has been recommended for multiple and recurrent lesions in some reports13,15,16,19). Spontaneous regression has also been reported5,17). Furthermore, lesions decrease in size 1 to 3 months after the diagnosis and disappear in a period of 3 to 19 months. In cases of decreasing size during the follow-up period, spontaneous regression can be expected. Longer follow-ups have revealed a local recurrence rate of 6% and a distant recurrence rate of 22%7,19,20). Therefore, follow-up evaluations for several years have been recommended.
CONCLUSION
The exact etiology of EG is unclear. Head trauma is regarded as an etiology. In the present case, minor trauma without hemorrhage or fracture can trigger the development of EG. The interval from the trauma to EG occurrence was 9 months, and this was quite a long period compared to previous reports. For pediatric patients, clinicians should be aware of a possible association between solitary EG of the skull and minor head trauma.