INTRODUCTION
Central hyperthermia is defined as high body temperature usually caused by stroke, and it responds poorly to antipyretic treatments. Prolonged central hyperthermia that develops from stroke is associated with a high risk of morbidity and mortality2,4,6,10,16-18). We report a rare but successful case of management of a patient with central hyperthermia, which occurred after intracerebral hemorrhage (ICH) in the basal ganglia with baclofen.
CASE REPORT
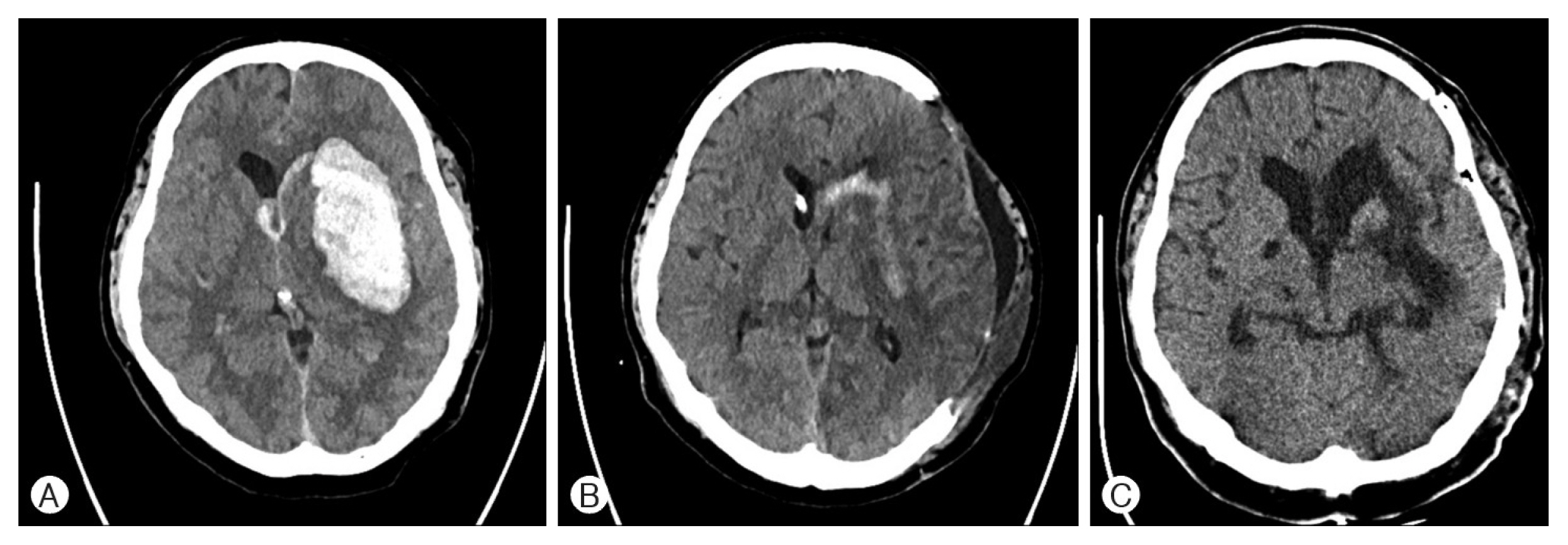
A 35-year-old man with no medical history presented to the emergency room with sudden loss of consciousness (Glasgow Coma Scale, E1V1M4) and right-sided hemiplegia on neurologic examination. Non-contrast computed tomography (CT) demonstrated acute left basal ganglia hemorrhage with a midline shift (Fig. 1A). The patient was treated with emergency decompressive craniectomy and hematoma evacuation (Fig. 1B). Post surgery, he was admitted to the intensive care unit and managed with mechanical ventilation with monitoring systems and medication. On postoperative day (POD) 12, he presented with intermittent fever and sudden muscle rigidity. Despite thorough diagnostic evaluation to rule out the focus of infection and full coverage of broad-spectrum antibiotics, the fever persisted and fluctuated in the range of 38.2°C to 39.6°C. Routine biochemistry and hematological tests showed no evidence of inflammation with a normal white blood cell count (7,900/mL), C-reactive protein level (5.3mg/L), and negative blood culture results. The anticoagulation tests and lumbar puncture cerebrospinal fluid analysis on POD 16 were normal (red blood cells, 220/mm3; white blood cells, 5/mm3; glucose, 71mg/dL; and protein, 51mg/dL). He showed no signs of active inflammation, and his coagulation test results were normal; therefore, it could be concluded that central hyperthermia was the likely cause of the prolonged fever. Central hyperthermia was treated with baclofen at a dose of 30mg/day on POD 18, and the dose was increased to 60mg/day on POD 22. Hyperthermia did not subside when the dose of baclofen was 30mg/day; however, the body temperature fluctuated between 39°C and 37°C on POD 23 but did not reach the normal level. On POD 30, we increased the baclofen dose to 90mg/day, and the body temperature was reduced to normal levels. The neurological state showed gradual improvement with a reduction in stupor and muscle rigidity. Postoperative CT demonstrated resolved ICH without any midline shift (Fig. 1C). Postoperative magnetic resonance imaging demonstrated encephalomalacia due to ICH in the left frontotemporoparietal lobe, basal ganglia, external capsule (Fig. 2).
DISCUSSION
Central hyperthermia is characterized by a cytokine-related elevation setting of the thermoregulatory center that fails to respond to antipyretic treatments. The diagnostic criteria for central fever are not standardized and there are different opinions regarding the time of fever onset, but we used the following criteria to diagnose central hyperthermia: (1) no prior infection or fever for at least one week before onset of stroke; (2) presence of fever (≥38.3°C) after onset of stroke; and (3) negative workup for infection-originated fever5,7,9). Early diagnosis and treatment of central hyperthermia are crucial. However, in most cases, early diagnosis is difficult because of the time-consuming tests required to rule out infection. Furthermore, the mortality rate is high because of complications related to high fever, including sudden cardiac arrest, rhabdomyolysis, and acute renal failure9). The precise mechanism of central fever in stroke remains unknown. Body temperature is strictly controlled in the human body. Multiple physiological mechanisms are involved in thermoregulation, all coordinated with the cutaneous thermal receptors, spinal cord, midbrain, and thermoregulatory center of the hypothalamus13). Several possible mechanisms can explain central hyperthermia. First, the central pathway controls thermoregulatory thermogenesis and innervation of the brown adipose tissue (BAT). The BAT is an essential effector organ for nonshivering heat generation that helps maintains euthermia during exposure to cold19). Preoptic chiasma and anterior hypothalamic nuclei are the centers of thermoregulation. Lowering the temperature of these areas activates the BAT, while raising the temperature deactivates the BAT and nonshivering thermogenesis11,15). Preoptic chiasma/anterior hypothalamic nuclei generate efferent signals that reach the ventromedial hypothalamic nuclei and act as γ-aminobutyric acid (GABA) inhibitors12). Signals from the ventromedial hypothalamic nucleus reach the raphe nuclei through the lower midbrain, releasing GABA from this region14). The thermoregulatory signal is connected to the sympathetic chain, and the nonshivering thermogenesis in the BAT is controlled by the sympathetic chain7,9). Second, dysfunction of the serotonergic or dopaminergic system can also be a possible cause of central hyperthermia; the serotonergic system is associated with heat generation, while the dopaminergic system is associated with autonomic and endocrine regulation18). Symptoms of central hyperthermia are thought to be related to dopamine or serotonin syndrome, including hyperthermia, altered mental state, muscle hypertonia, and autonomic dysfunction. These symptoms are similar to those of our patient who had hyperthermia, altered mental state, and muscle hypertonia. Lastly, the correlation of the central fever with the ICH volume and third ventricular shift suggests possible hypothalamic compression after ICH. Previous studies found no significant correlation between the ICH location and development of central hyperthermia, although thalamic and basal ganglia involvement showed a trend towards being more common in patients with central hyperthermia4,6).
The precise mechanism of action of baclofen is not fully known; however, thus far, baclofen is an agonist of the beta subunit of GABA receptors on mono- and polysynaptic neurons at the level of the spinal cord and brain1). Regarding the antipyretic effect, we hypothesized two mechanisms of action by which baclofen possible lowered the body temperature. First, baclofen, a GABA receptor agonist, replaces GABA, thereby directly inhibiting the raphe nuclei and suppressing BAT activation, while GABA is blocked because of the mass effect of ICH7). Baclofen lowers the body temperature by affecting the dopaminergic system. According to a previous study, low concentrations of baclofen caused increased activity of dopaminergic neurons in rodent ventral tegmental area slices3). As the symptoms of our patient were related to dopamine deficiency, baclofen’s action of increasing the activity of dopaminergic neurons may lower the body temperature of the patient. However, this hypothesis can be controversial because, in this study, higher doses of baclofen inhibited dopaminergic neurons, which usually raises the body temperature, but our patient’s body temperature decreased as the dose of baclofen was increased.
CONCLUSION
This case provides guidance for understanding the thermoregulation dysfunction in patients with ICH. Thus, in conclusion, persistent central hyperthermia should be considered as a possible cause of fever in patients with ICH, and baclofen administration should be considered as a treatment option.