INTRODUCTION
Nerve transfer to restore nerve function following traumatic avulsion injuries has been described previously. However, there is still a paucity of literature regarding the technique and long-term outcomes of these procedures. Double fascicular nerve transfer (DFNT) involves ulnar and median fascicular transfers to the musculocutaneous nerve to restore elbow flexion. This technique was introduced by Liverneaux et al. in 2006 using double donor fascicles, which are flexor carpi ulnaris (FCU) and flexor digitorum superficialis (FDS); the procedure now used is called the Oberlin technique 2, and is performed in patients with traumatic nerve injury without motor improvement.
Neuralgic amyotrophy (NA) is a distinct clinical syndrome of unknown etiology involving the brachial plexus, which is characterized by the acute onset of shoulder and arm pain followed by weakness and sensory loss. NA, known as Parsonage-Turner syndrome, is a rare immunologic or inflammatory disorder characterized by paresthesia and sporadic non-dermatomal motor weakness. To date, there is no unified treatment paradigm. Patients with NA usually recover spontaneously without sequelae. However, motor weakness may not be completely restored in some cases. The authors performed DFNT in a patient with NA to restore elbow flexion. This study aimed to investigate the short-term outcomes and feasibility of DFNT applied to non-traumatic neuropathy.
CASE REPORT
A 63-year-old male, right-handed, presented to us with a 1-month history of monoparesis of the right upper extremity. This was preceded by acute sharp pain in the periscapular area lasting for three days. The patient had no history of trauma or known musculoskeletal conditions. On neurologic examination, the patient had a prominent weakness with atrophy of the right shoulder. On the Medical Research Council (MRC) scale, shoulder abduction had a grade of 1/5; elbow flexion, 0/5; elbow extension, 3/5; wrist flexion, 2/5; wrist extension, 3/5; and hand grasping, 2/5.
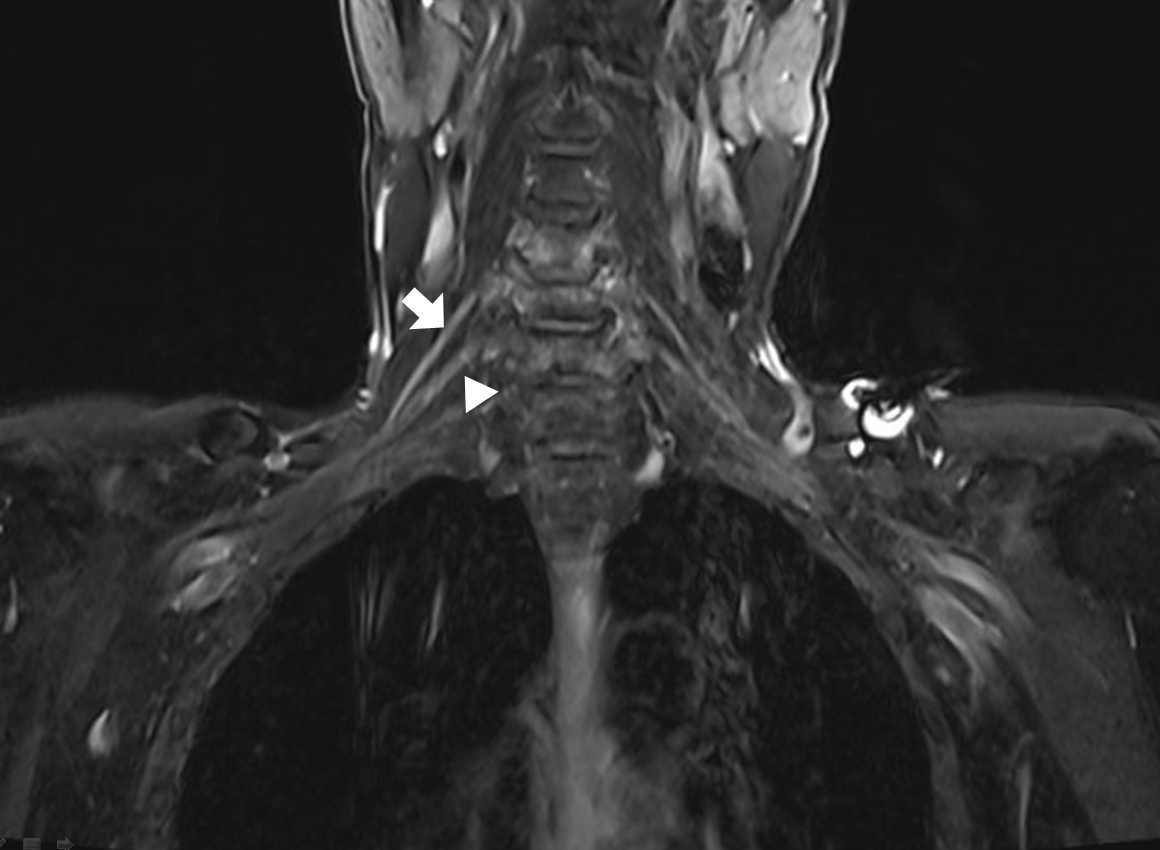
Electromyography was suggestive of pan-brachial plexopathy. Magnetic resonance neurogram of the brachial plexus demonstrated swelling at the post-ganglionic level of the C5 and C6 nerve roots with high signal intensity and muscle atrophy (Fig. 1). The patient was diagnosed with NA.
The pain resolved spontaneously without intervention. The patient was discharged with recommendations for active physiotherapy to restore muscle strength. However, the patient was lost to follow-up because of economic constraints. He was seen again 23 months later for persistent elbow flexion weakness. On examination, shoulder abduction had a grade of 3/5 but elbow flexion had a grade of 0/5. Elbow extension, wrist flexion/extension, and hand grasping were restored to normal strength (Supplementary Video 1).
DFNT was performed. An incision was made along the brachial sulcus. The medial intermuscular septum was dissected to identify the musculocutaneous nerve. The brachialis and distal biceps brachii motor branches were selected as the recipient nerves. Moving inferiorly, we identified the median nerve, performed internal neurolysis, and selected the motor branch of the FDS as a donor fascicle. The ulnar nerve was similarly separated, and the motor branch of the FCU was selected as a donor fascicle. We used an intraoperative nerve stimulator (ISIS IOM system; inomed Medizintechnik GmbH, Emmendingen, Germany) to confirm the FDS and FCU. After individual fascicular mapping, the donor fascicles were coapted on the recipient fascicles: the FDS to biceps brachii; FCU to brachialis (Fig. 2).
Postoperatively, he complained of paresthesia in the ulnar distribution and difficulty with right-hand clumsiness. Ten days later, biceps muscle contraction was revealed, and on the fourteenth day, grade 3 elbow flexion strength was identified (Supplementary Video 2).
DISCUSSION
Restoration of elbow flexion is the main goal of treatment in patients with brachial plexus palsy involving the upper trunk7,8). Nerve grafts and repair were historically performed by direct exploration of the injury site at the level of the brachial plexus. Recently, a nerve transfer technique was introduced, in which a healthy nerve was connected to a damaged nerve for regeneration. The main focus was on the area adjacent to the affected muscle innervated by the target nerve to be restored. In 1994, Oberlin et al.9) introduced a nerve transfer method, the Oberlin 1 technique, that connects the motor branch of the ulnar nerve to the biceps branch. Improvement of elbow flexion was document in his first report.
A recent paper reported only modest improvements with this method. Out of 11 patients with brachial plexus injury (BPI) during childbirth, only 4 patients showed improvement with MRC grade 3 or higher compared to Oberlin’s initial results; the follow-up period was up to 10 years4). In 2006, Liverneaux et al.5) introduced the DFNT, named Oberlin 2, for elbow flexion restoration, adding a synergistic fascicle to the donor nerve. In this technique, donor nerves from the motor fascicles of the median and ulnar nerves were connected to the motor branch of the biceps brachii and the motor branch of the brachialis from the musculocutaneous nerve. DFNT was performed in 10 of 15 patients with BPI who had not improved for 6 months. All 10 patients showed improvement in muscle strength with an MRC grade 4. The surgical method of nerve transfer for elbow flexors is commonly referred to as Oberlin 1 or 2, with clinical improvement reported at 6 months to 12 months postoperatively. One case report described improvement 6 months after DFNT in a patient with radiation-induced brachial plexopathy. The patient had external beam radiation for breast cancer 12 years prior to biceps weakness13). Case reports of DFNT in patients with NA are rare.
In our case, the patient had complete paralysis of elbow flexion secondary to NA, and was treated with the Oberlin 2 DFNT. Muscle contraction of the brachialis was observed from day 10 after surgery, and recovery of MRC grade 3 of elbow flexion was observed from day 14 after surgery.
In general, nerve transfers recover relatively quickly compared to nerve grafts, which is reported to be one of the most important factors in the number of viable motor axons1,10,12). This technique allows the transfer of regenerating motor axons very close to the neuromuscular junction of the elbow flexors, minimizing the distance and time required for the regenerating front to reach the target muscle2,10-12,14). Therefore, patients with prolonged onset of disease can also be candidates for this procedure.
Although the musculocutaneous nerve also regenerated to some extent in our case, it is believed that the number of motor axons was insufficient to reach a functional state. Immediately after surgery, the paresthesias in the ulnar distribution and hand clumsiness reported could be attributed to traction of the ulnar nerve. The patient recovered gradually and spontaneously recovered without further intervention. DFNT surgery would not have been attempted in this patient if the median and ulnar nerve functions would have restored to only MRC grade 4 or lower.
In addition, the therapeutic benefit of nerve transfer in trauma-related BPI is often time-dependent. Hence, tendon transfer is recommended when muscle atrophy is already advanced. Although spontaneous recovery is related to the mechanism of injury, it is more common in low-energy trauma than in high-energy3,6,11,13). This is believed to be determined by a sufficiency of viable axons in the musculocutaneous nerve required for elbow flexion. Although this was not enough to flex the elbow, the recipient nerve was relatively healthy, leading to good short-term outcomes.
In conclusion, we suggest that the DFNT may be a safe and effective method to restore elbow flexion in patients with NA.