INTRODUCTION
Transforaminal lumbar interbody fusion (TLIF) is an effective operative procedure, showing satisfactory results with acceptable risk rates16). It has gained popularity due to its minimal invasiveness, lower blood loss compared to other surgical techniques, and shorter hospitalization period8). Ironically the increase in the popularity of TLIF has also resulted in increased complication rates, including dural tears, nerve root injuries, screw loosening, and cage mispositioning or migration. Here, we present a rare case of the intraoperative anterior extrusion of a fusion cage during TLIF.
CASE REPORT
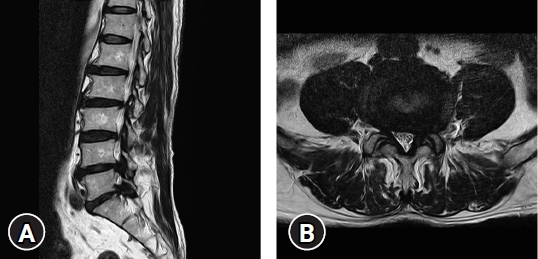
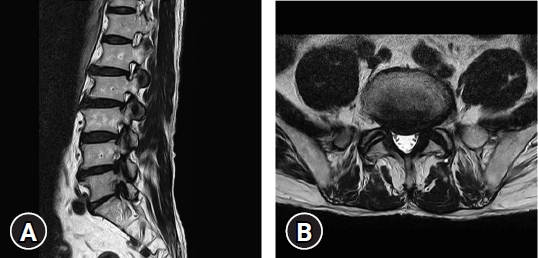
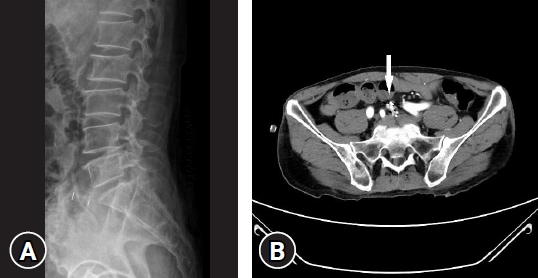
A 76-year-old male patient had initially experienced a gradual aggravation of left lower extremity motor weakness and radiating pain in the L5 and S1 dermatome. His imaging workup carried out at a local spine center, showed severe left L4-5 and L5-S1 foraminal stenosis with central disc extrusion and spondylolisthesis at L5-S1 level (Fig. 1, 2). The patient underwent open lumbar microdiscectomy at the L4-5 level and TLIF at the L5-S1 level. Unfortunately, during the cage insertion procedure at the L5-S1 level, anterior migration occurred where the cage disappeared into the abdominal space. The patient was immediately transferred to our hospital for a thorough evaluation and possible emergency surgery. The patient was very stable when he arrived at our emergency room and his initial symptoms had subsided. Imaging workup X-rays and computed tomography angiography (CTA) (Fig. 3) revealed no major vessel injuries, and the lost cage was placed just below the iliac artery bifurcation area. The patient was hemodynamically stable and was sent to the intensive care unit.
With the help of the department of general surgery, anterior lumbar body fusion (ALIF) at L5-S1 was performed the next day to both remove the migrated cage and restore stability to the lumbar spine. In the surgical field, the cage was located in front of the L5-S1 disc space just below the iliac artery bifurcation, and no bleeding or vessel injury was observed (Fig. 4). The cage was removed, and a large ALIF cage was inserted without any complications. Then, the patient was placed in the prone position, and pedicle screws were inserted percutaneously.
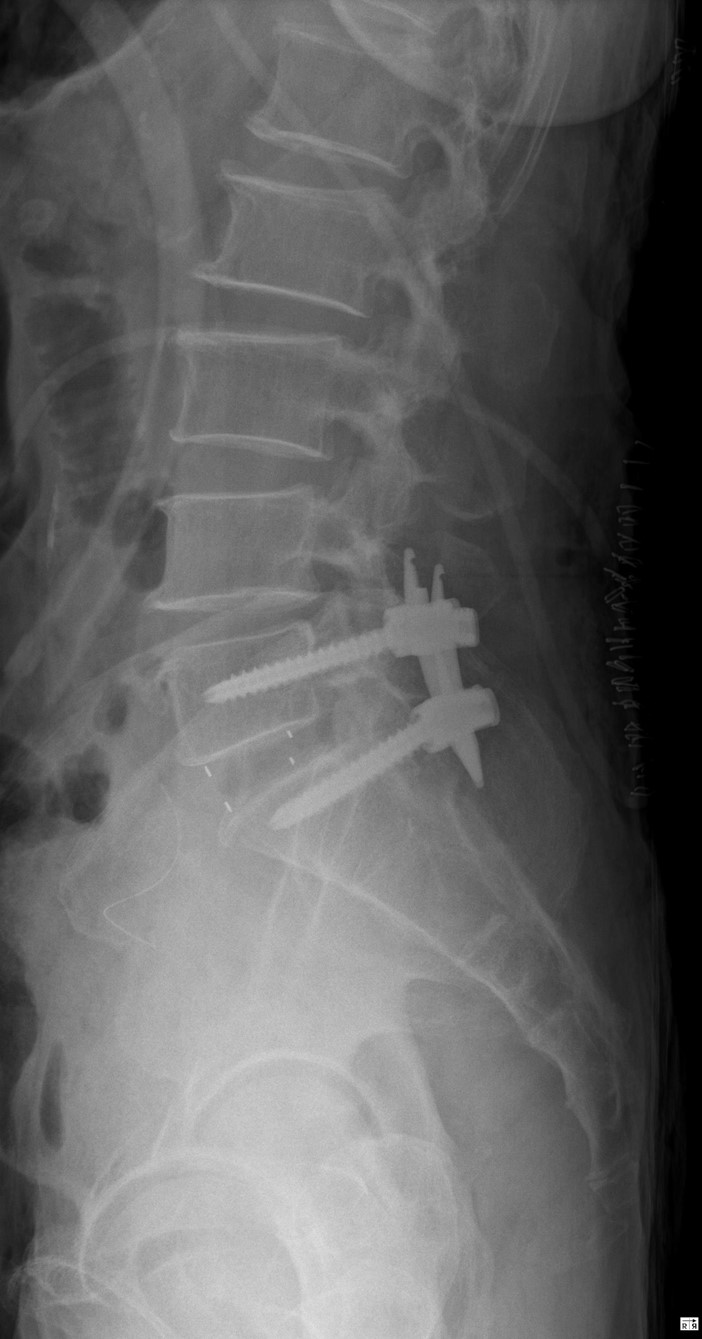
Surgery was completed successfully without complications (Fig. 5). The patient was discharged ten days after surgery with no neurological deficits.
DISCUSSION
TLIF surgery was first introduced in 1982 by Harms and Rolinger6), and it is considered the preferred method of interbody fusion. There are several advantages of TLIF compared to previous conventional methods of spine interbody fusion. TLIF minimizes the possibility of dural and nerve injury since only minimal thecal sac traction is needed for cage entry after the removal of the ipsilateral facet. Also, through the removal of the facet, the problematic foraminal area can be exposed with little difficulty. Another benefit of TLIF is that additional posterolateral fusion is possible since the contralateral laminae and spinous processes are usually preserved4).
However, even with these excellent features of TLIF, critical complications can occur during the procedure. Although rare, as the case presented in this study, one of the most infamous complications is anterior cage migration. Anterior migration during the procedure can occur when the operator is inserting the cage into the disc space. During this process, the surgeon’s excessive curettage and strong impaction can result in an anterior longitudinal ligament (ALL) tear leading to instant anterior migration into the abdominal space. This could lead to major vessel injuries, resulting in catastrophic consequences3). Many studies have reported the risk factors of cage migration, such as old age, low bone quality, small or oversized cages, and rectangularly shaped cages1,7-10,12,13,17,21). However, these factors are usually related to postoperative migration during the follow-up periods after successful surgery9,21). The preservation of the ALL during disc preparation is especially crucial during TLIF. The ALL usually acts as a barrier during the cage insertion process and minimizes the possibility of the cage entering the abdominal space. It attaches firmly to the anterior surface of the vertebrae. It is not strong on the lateral side which makes it more vulnerable to unilateral and oblique disc procedures than other operations11).
There are no guidelines for reoperation due to anterior cage migration. Although it would be reasonable to consider removing a foreign body that has the possibility of becoming an infection source or a possible cause of delayed vessel injury, there are many arguments against the removal of a migrated cage, especially in hemodynamically stable patients1,2,7,10,14,15,19,20) (Table 1).
CONCLUSION
TLIF is an increasingly popular procedure for lumbar interbody fusion, and it is mostly recommended for patients with unstable unilateral foraminal stenosis. Although TLIF is a common surgical procedure, it has possible severe complications and should not be taken lightly. Cage migration occurs in 1.8% of the patients and among them, anterior cage migration can cause lead to disastrous consequences18). Physicians should always take into account the possibility of anterior migration and try to preserve the ALL during disc preparation to reduce the chance of this critical complication.