Decompressive C1 Laminectomy without Fusion for the Treatment of Craniovertebral Junction Stenosis with Myelopathy: Could It be One of Option?
Article information
Abstract
Objective
Trans-oral approach or occipitocervical/atlantoaxial fusion with/without posterior decompression has been considered to be an appropriate surgical strategy for craniovertebral junction (CVJ) stenosis with myelopathy. However, decompressive C1 laminectomy without posterior stabilization was reported recently for treating retro-odontoid pseudotumor. This study aimed to evaluate surgical outcomes of the patients treated with decompressive C1 laminectomy without posterior stabilization for CVJ stenosis with myelopathy.
Methods
Ten patients underwent decompressive C1 laminectomy without posterior stabilization for CVJ stenosis with myelopathy from August 2007 to December 2016. All patients were evaluated preoperatively for spinal canal stenosis, cord signal changes, and instability based on preoperative computed tomography, magnetic resonance imaging, and plain dynamogram. We retrospectively reviewed the clinic charts and radiographs for investigating clinical outcomes such as the visual analog scale (VAS), and Ranawat grade scale and complications. Radiographic parameters including pre- and postoperative atlas-dens interval change in flexion and extension, O-C2 angle, C2-C7 Cobb angle, and C2-C7 sagittal vertical axis were measured.
Results
The mean follow-up time was 41 months. Eight men and 2 women with a mean age of 58 years (range, 45-69 years) were enrolled. Preoperative neck pain by the VAS was improved significantly in all patients (p<0.01). Nine of 10 patients showed improvement on the Ranawat grading scale, but 1 patient who required a Halo-vest due to aggravated instability after surgery remained unchanged. The statistical results of the preoperative and postoperative radiographic measurements were not significant.
Conclusion
In select patients with certain indications, decompressive C1 laminectomy could be a viable option, especially in the elderly, patients with comorbidity, and patients with poor bone quality.
INTRODUCTION
Craniovertebral junction (CVJ) stenosis with myelopathy has a significant detrimental impact on patient quality of life, and can produce severe neck pain, quadriparesis, and respiratory dysfunction. Patients with untreated CVJ stenosis are less likely to survive long-term and may be bedridden [18]. Patients with nonsurgical and conservative treatment had worse activities of daily living scores and were completely bedridden or deceased by the time of the final follow-up examination [16]. Surgery contributes to prolonging the life span, improvement of pain and quality of life, and reversal of neurological deterioration [15].
CVJ stenosis has been considered a secondary spinal event related to primary instability at the atlantoaxial joint [5,9,21]. Based on this proposed biomechanical mechanism of CVJ stenosis, the surgical methods considered are decompression or fusion. Therefore, the majority of surgeons have selected the trans-oral approach or occipitocervical/atlantoaxial fusion with or without posterior decompression, which has been considered an appropriate surgical strategy for CVJ stenosis [1,2,4,11]. These surgical methods have a high mortality rate in early postoperative period of 4% to 17% [14,15]. In addition, problems such as loosening of screws, complications due to prolonged operative time, limitation of neck movement, and adjacent segment degeneration can occur. This can be a major issue for the elderly, especially those with underlying comorbidities or poor bone quality.
Recently, some surgeons have reported decompressive C1 laminectomy without posterior stabilization [10,19]. So far, the C1 laminectomy without posterior stabilization method has been performed only in retro-odontoid pseudo-tumor. We considered a simple decompressive laminectomy without posterior stabilization method in patients with CVJ stenosis with myelopathy, which is especially associated with instability, to provide longterm preserved stability. Thus this could be an additional option for surgical treatment in the elderly patient or patient with severe comorbidity. This study was designed to evaluate the clinical and radiographic outcomes of patients treated with decompressive C1 laminectomy without posterior stabilization for CVJ stenosis with myelopathy for over 3 years follow-up.
MATERIALS AND METHODS
1. Patients
This study was approved by our Institute Review Board. From August 2007 to December 2016, we performed decompressive C1 laminectomy without posterior stabilization for CVJ stenosis with myelopathy in 10 patients. All patients were evaluated preoperatively for spinal canal stenosis, cord signal change, and instability based on preoperative computed tomography, magnetic resonance imaging, and plain dynamogram. We retrospectively reviewed the clinic charts and radiographs for investigating clinical outcomes such as patient age, sex, neck and arm pain by visual analog scale (VAS), clinical symptoms, and complication. Preoperative and final follow-up neurological were graded on the Ranawat scale [17] (Tables 1, 2).
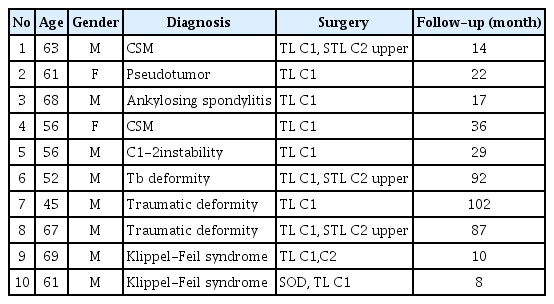
Summary of patient demographics
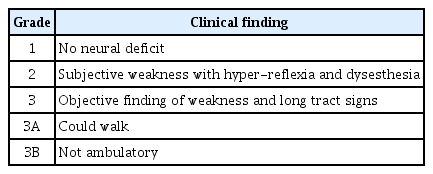
Ranawat scale of the patient impairment with spinal cord compression
Radiographic parameters including pre- and postoperative atlas-dens interval (ADI) change in flexion and extension, occipito-C2 angle (O-C2A) angle (O-C2A), C2-C7 Cobb angle, and C2-C7 sagittal vertical axis (SVA) were measured. The O-C2A, C2-C7 Cobb angle, and C2-7 SVA parameters have been documented elsewhere [3,8,13] (Fig. 1). Briefly, the O-C2A indicates the angle between McGregor’s line and the inferior vertebral endplate line of C2. The C2-C7 Cobb angle indicates the angle between the inferior endplates of the C2 and C7 vertebral bodies. If the C7 vertebra was included in the fused vertebrae, we used the C2-end vertebrae of the fused segments below the C7 angle for analysis. In both measurements, a positive value indicates lordosis at the local segment.
Occipito-C2 anglewas defined as the angle between McGregor’s line(a) and the inferior endplate line in the C2(b), and C2-C7 Cobb angel measured between the interior endplate of C2(b) and C7(c). The C2-C7 sagittal vertical axis was defined as the deviation of the C2 plumb line(d, extending from the centroid of the C2 vertebra) from the posterior superior end plate of C7 (e).
The differences in ADI are defined as the differences between the values in flexion and value in extension. Regarding surgical factors, we evaluated operation time, blood loss, and intraoperative complications.
2. Statistical Analysis
The operation was performed with the patient in the prone position. The C1 laminectomy range was just before both lateral masses of the C1 lamina. In 3 of 10 patients, Partial additional C2 laminectomy was needed. If the fibrous adhesive band is still noted to be compressing the spinal cord intraoperatively, it should be removed after laminectomy. Following surgery, a Philadelphia neck collar was used for all patients for 3 months postoperatively. Additionally, patients were instructed to be careful about excessive flexion, extension, and impact.
RESULTS
1. Clinical Outcomes
The mean follow-up time was 41 months. Eight men and 2 women with a mean age of 58 years (range, 45-69 years) were included in this study. Pre- and postoperative VAS was used to evaluate for neck pain and significantly improved from a mean 5.8 to a mean 1.8 after surgery (p<0.01). Nine of 10 patients showed improvement on the Ranawat grading scale, but 1 patient remained unchanged (Ranawat grade IIIb). The patient showed a preoperative ADI in flexion of 9.55 mm, extension of 2.7 mm, and a 6-month postoperative ADI of 11.56 mm and 11.17 mm, respectively. Eventually, the patient required a Halo-vest due to aggravated instability (Table 3).
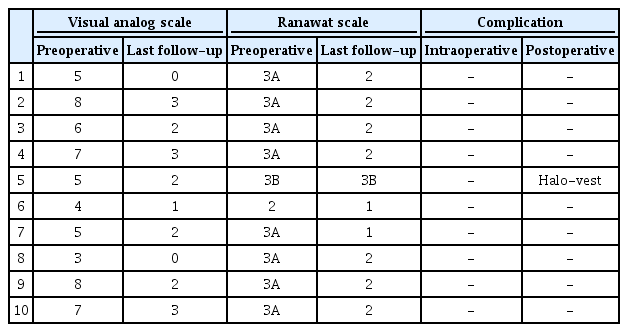
Result of surgical treatment
2. Radiologic Outcome
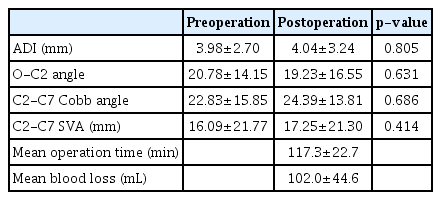
Atlantoaxial instability was defined as an ADI >4 mm, according to the criteria described by White and Panjabi. The number of patients with an ADI in flexion >4 mm was 3 before surgery and 4 after surgery in this study. The number of patients showing a difference between flexion and extension in ADI of >3 mm was 3 before surgery and 2 after surgery. The average OC2 angle was 20.78° preoperatively and 19.23° postoperatively, and the preoperative and postoperative difference was 1.55°. The mean C2-C7 Cobb angle was 22.83° preoperatively and 24.39° postoperatively, and the preoperative and postoperative difference was -1.56°. The preoperative C2-C7 SVA mean was 16.09 mm and postoperative mean was 17.25 mm. The statistical results of the preoperative and postoperative radiographic measurements (ADI, OC2 angle, C2-C7 Cobb angle, and C2-C7 SVA) showed no significant differences. The mean surgical time was 117.3±22.7 min, and the mean blood loss was 102±44.6 mL. There was no documentation of surgical complication such as dura tear, vertebral artery-related injury, and intraoperative cord injury in any patient during the postoperative course (Fig. 2, Table 4).

A 68 year-old man. Cervical stenosis with cord signal change was revealed by sagittal image on T2-weighted magnetic resonance imaging (A). Follow C1 laminectomy (B), cord compression is released (D). Preoperative (C, D) and postoperative (E, F) lateral dynamic radiographs that were obtained in the flexion (C, E) and extension (D, F). Comparing preoperative and postoperative dynamic radiographs, (C, E) vs. (D, F), additional atlantoaxial instability is not seen.
Radiologic and intraoperative outcomes
DISCUSSION
The CVJ is the most mobile area of the human body. The CVJ is composed of 3 components: bone (occipital bone, atlas, and axis), joint, and circumjacent ligaments. The relationship between these components is complex and difficult to understand. The CVJ protects the cervical spinal cord, brain stem, and lower cranial nerves, and concurrently provides excellent flexibility in the O-C1 and C1-2 joints. Specifically, the O-C1 joint represents 50% of the total flexion-extension motion in the entire cervical spine, while the C1-2 joint accounts for 50% of the rotational motion [10,20]. The ligaments are the main contributor to mechanical stability of the CVJ. The transverse and alar ligaments attaching to the posterior odontoid process are especially important to control the CVJ. The posterior occipito-atlantal membrane and posterior atlantoaxial membrane are attached to the posterior arch of the atlas; however, these membranes are less important than the transverse and alar ligaments for stabilizing the CVJ biomechanics. The degeneration of the articular cartilage, reduction in joint space, and secondary incompetence of ligaments controlling movements probably lead to atlantoaxial instability [4,7,12]. Atlantoaxial joint arthritis is likely initiated or exacerbated by a subtle trauma. The clinical features suggest that the process of joint degeneration and instability are progressive phenomena and extend over several months to years.
Regarding these pathobiomechanical causes and concerns about increased instability, CVJ stenosis has been treated with the posterior stabilization method. The posterior stabilization method for CVJ stenosis is the most common treatment, but it has distinct disadvantages, such as the need for instrumentation, morbidity due to bone grafting, a restricted range of neck movement, dyspnea, and dysphagia [6,13,22]. As observed in this study, C1 decompressive laminectomy without posterior stabilization shows satisfactory clinical, neurological, and surgical outcomes without severe complication.
While CVJ stenosis is often associated with ossification of anterior longitudinal ligament, ossification of posterior longitudinal ligament, and severe cervical spondylosis, the cervical range of motion (ROM) of patients with CVJ stenosis is fundamentally disturbed. A posterior fusion would lead to further reduction in ROM, and thus should be avoided. Based on these anatomical properties and the results of this study, C1 laminectomy without posterior stabilization method is not considered to induce postoperative atlantoaxial instability. Rather, it produced rapid recovery in its short operation time and reduced operative bleeding, and patients showed neurological and clinical improvement.
On the other hand, it is crucial to maintain stability in C1 laminectomy without posterior stabilization because long-term degenerative changes such as facet hypertrophy or fusion that result in restabilization of existing structures may occur. In the same manner, several radiological indexes implying instability-basion-axial interval less than 12 mm, basion-dens interval less than 9 mm, atlanto-occipital interval less than 4 mm, ADI over 3 mm, flexion/extension ADI difference over 9 mm - are generally considered more suitable for occipitocervical fusion.
Therefore, although the exact indication is not yet defined, we could expect that patients with old age, combined comorbidity, poor bone quality, posterior compression as their main problem and previous chronic degenerative changes enough to prevent instability could be good candidates for C1 decompressive laminectomy without posterior stabilization. However, longer-term follow-up is needed to assess the potential instability of the CVJ. One patient needed additional treatment after surgery, but this patient may not have had the proper indications. Considerable instability existed preoperatively but was neglected in case of revisional additional fusion after C1 laminectomy. The revision surgery was not difficult as only fixation and fusion is needed.
Recently, 2 publications have reported patients with retroodontoid mass lesions that were treated with C1 laminectomy without posterior stabilization [10,19]. They also showed good clinical and neurological outcomes without resultant atlantoaxial instability. Considering these study results, C1 decompressive laminectomy without posterior stabilization may be an effective and safe surgical alternative. In our study, the final follow up results showed good clinical and neurological outcomes in all patients except for one, in whom a Halo-vest was required. Regarding atlantoaxial instability, instability progression was observed in 1 of 10 patients, although this did not result in any clinical issues and neurological outcome improved. These good clinical and neurological outcomes show the suitability of this surgical option in treating this pathology.
There are some limitations of this study. Selection bias and a small group are the primary limitations, as the study was a retrospective chart review of 10 patients. In the future, an analysis of risk factors for aggravation of postoperative instability should incorporate a large number of patients. Providing biomechanical evidence for C1 laminectomy without pos- terior fusion and its effect on instability is necessary. In addition, the appropriate indications for the surgical plan are crucial, and thus prospective randomized studies will be needed in the future.
CONCLUSION
Surgical intervention remains the most effective therapeutic option for patients with CVJ stenosis with myelopathy. In this study, patients showed improvement in clinical and neurological outcomes, even when presenting preoperatively with atlanto-axial instability. In select patients with certain indications, decompressive C1 laminectomy without posterior stabilization could be viable option, especially in elderly patients, and patients with comorbidity and/or poor bone quality.
Notes
No potential conflict of interest relevant to this article was reported.