Relationship between Estrogen Hormone and Rupture of Cerebral Aneurysm in Premenopausal Women
Article information
Abstract
Objective
The incidence of subarachnoid hemorrhage (SAH) in women increase after menopause. Estrogen hormone had been implicated in cerebral aneurysm formation, growth and rupture. The aim of this study was to examine the association between estrogen hormone and presence of aneurysmal SAH in premenopausal women.
Methods
Between February 2015 and December 2016, 40 patients at consecutive premenopausal women (mean age, 41 years) with aneurysms SAH, were treated in our hospital. The data of patients with clinical and gynecological history were analyzed and compared with control group with age matched, case-control study.
Results
Single and multivariate analysis showed that estrogen hormone (estradiol) had a lower trend towards at premenopause age comparing with control group, statistically was significant (p<0.001). No significant association of SAH was found with gynecological and clinical factors (p>0.05).
Conclusion
In our study, there is a trend showing that an earlier age at menopause relating to estrogen hormone deficiency is associated with the aneurysmal SAH. These data may help to identify a risk factor for pathogenesis of cerebral aneurysm and also a potential target for future therapies.
INTRODUCTION
The cerebral aneurysm is a prevalent acquired cerebrovascular disease that can cause a catastrophic subarachnoid hemorrhage (SAH). Mortality rates for aneurysmal SAH continue to average near 50%, with 10% of patients dying before ever reaching the hospital and approximately 20% sustaining severe disability [1,6,7,18,29,32]. Unlike most other types of cerebrovascular disease, SAH occurs more frequently in women than in men. Mortality rates of female SAH patients have been reported to be higher than those for men [2,3,8,9,15,16,19,23,25,32,33].
Despite the catastrophic consequence of aneurysmal SAH, very little is understood regarding their pathogenesis, and there are no reliable predictive markers for identifying risk aneurysm rupture. Previous studies have addressed the molecular pathological basis and mechanisms of intracranial aneurysm formation, growth, and rupture. The formation, growth, and rupture of cerebral aneurysms have been associated with inflammatory processes, and these have been implicated in the digestion and breakdown of vascular wall matrix. Remodeling of the vascular extracellular matrix has been found to be involved in the pathogenesis of cerebral aneurysm like aortic aneurysm, atherosclerosis, and arteritis [4,12,14,26,31,34]. The potential mechanism by which estrogen hormone protects against cerebrovascular events, however, is less understood.
A growing body of evidence indicates that the risk of aneurysm formation and SAH in women rises after menopause. The loss of estrogen earlier in a woman’s life may contribute to the pathogenesis of aneurysm formation and SAH. Because the incidence of SAH is higher after menopause than before, it has been suggested that the estrogen hormone might be protective against the aneurysm formation and SAH [5,10,11,17,20-22,27,28,30]. However, the benefit of postmenopausal estrogen hormone replacement therapy (HRT) for aneurysm formation and rupture is not clear [13,21,24,35]. We hypothesize that decreases in both circulating estrogen hormone level and cerebrovascular estrogen hormone receptor density may contribute to an increased risk of aneurysm formation and rupture.
Considering above mentioned aspects, the aim of this study is to investigate the role of estrogen hormone in pathogenesis of aneurysm formation and rupture in patients with aneurysmal SAH. To accomplish this, we compared the study group of premenopausal women patients with aneurysmal SAH, with control group of age-matched premenopause women in the general public.
MATERIALS AND METHODS
1. Patients
Between February 2015 and December 2016, a total of 40 premenopausal women patients with aneurysmal SAH, were admitted in our hospital. They were with a mean age of 41 years and the clinical characteristics, locations of aneurysms of these patients are described in Tables 1 and 2. To define the role of estrogen in aneurysmal SAH, we compared data of the control group with that of the study group in the age-matched categories of <40, 40 to 44 and >45 years (Tables 3, 4). The exclusion criteria of patients for this study were postmenopausal women, patients with estrogen supplement therapy for cancer, not collection of blood sample of estrogen and patients with SAH of fusiform, traumatic, or mycotic aneurysm. To define role of estrogen for aneurysmal SAH, we compared with data of control group in the general public, which were matched with that of the study group for age in categories of <40, 40 to 44 and >45 years. This study was approved by our institution internal review board, and informed consent was obtained from family members. By measurement of estrogen hormone, all patients had blood samples drawn after onset of SAH. Plasma levels of estradiol (E2), was measured at a laboratory.
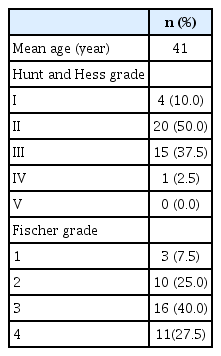
Patient characteristics (n=40)

Location of aneurysms (n=40)
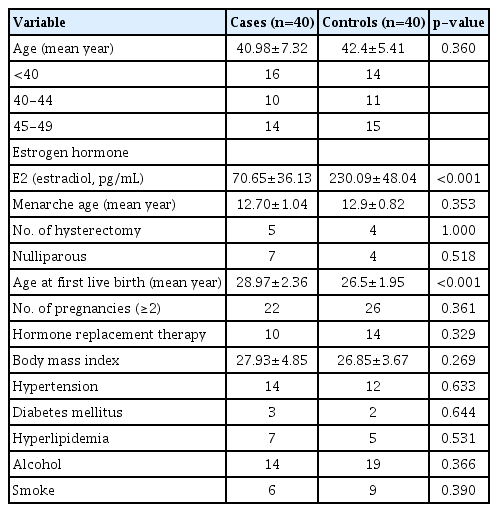
Univariate analysis of gynecological and clinical factors

Multivariate analysis of gynecological and clinical factors
2. Gynecological & Clinical Medical History
Age at premenopausal women was then subdivided into 3 premature menopause periods occurring at <40 years, 41 to 44 years, and 45 to 50 years. Patients were asked to provide the following information about their gynecological history: age at menarche, history of hysterectomy, parity or nulliparity, age at first live birth, number of pregnancies, and use of HRT. As part of their past clinical history, patients were asked to indicate whether they had ever been diagnosed with hypertension, diabetes mellitus, high cholesterol, body mass index (BMI; calculated as weight in kilograms divided by heights in meters sqared), alcohol and smoke history.
3. Statistical Analysis
The χ2 test was used to determine differences between the case and control groups for categorical values, while continuous values were examined with the student t-test. Univariate and multivariate analysis was performed to determine the association of aneurysmal SAH and risk factors. A p-value of less than 0.05 was considered significant.
RESULTS
A total of 40 consecutive premenopausal aneurysmal SAH patients and age-matched control groups were identified (mean age, 41±6.2 years and 42.4±4.8 years). Comparison of gynecological and clinical profile between study and control group, summarized in Tables 3 and 4. Compared with the control group, the study group showed no statistically significant difference in gynecological factors such as age at menarche, history of hysterectomy, parity or nulliparity, age at first live birth, number of pregnancies, and use of HRT. The clinical factors such as hypertension, diabetes mellitus, high cholesterol, BMI, alcohol and smoke also demonstrated statistically no significant difference in between study and control group. However, the study group showed a decreased trend towards premature menopause in level of estrogen hormone comparing with control group, which means this difference was statistically significant (p<0.001).
DISCUSSION
The previous studies have demonstrated the phenomenon of menopause on gender disparities in cardio or cerebrovascular disease appear to be at increased risk of developing of stroke comparing with men. Aneurysmal SAH occurs more frequently in women than in men, and mortality rates of female aneurysmal SAH patients have been reported to be higher than those for men [1,3,7,10,15,20,23,25,30,33]. Both female sex and the postmenopausal state were found to be significantly associated with the development of multiple cerebral aneurysms in patients as opposed to single aneurysms. Women had a significantly higher risk for de novo aneurysm formation than men in a long-term follow-up study, and being female was a significant independent risk factor for aneurysm growth. Additionally, it has been shown that faster aneurysm growth increases the likelihood of rupture [1,5-7,9,15,20,28,29,33]. And, premenopausal women study demonstrated that women who had gone through menopause at early ages showed a higher risk of stroke than those with menopause at late ages. That means that the loss of estrogen hormone that occurs at menopause has been cited as a central contributing factor to this increase in risk for postmenopausal women, a risk which is further exacerbated by early timing of the menopause. The loss of estrogen earlier in a woman’s life may contribute to the pathogenesis of cerebral aneurysm formation. Because the incidence of SAH is higher after menopause than before, it has been suggested that the sex hormones, especially estrogen, might be protective against the condition [1,2,4-7,9,13,16,17,20,28-30,32,33].
In animal studies, Jamous et al. [11] and Tada et al. [31] sought to elucidate the role of estrogen hormone in aneurysm formation by comparing rats or mice that had undergone oophorectomy with those that had not. Despite inducing cerebral aneurysms in all experimental rats or mice, the incidence of cerebral aneurysm formation in oophorectomized rats was found to be much higher than in rats with intact ovaries. These results subsequently indicated that estrogen hormone plays a protective role in the pathogenesis of formation of cerebral aneurysms.
Like all arteries, cerebral arteries consist of 3 layers: intima, media, and adventitia. The internal elastic lamina separates the intima from the media and is essentially a fenestrated sheet of elastin. Collagen fibers are mainly produced by fibroblasts. Fibroblasts also produce, organize, and remove the extracellular matrix. The repair and maintenance of connective tissue are performed predominantly by fibroblasts. The loss of media in the location of aneurysms is taken to be responsible for the initiation of aneurysm growth. The aneurysm is regarded as a development of the adventitia, which is composed of a layer of collagen fibers. The collagen fibers are the only load-bearing constituent in the aneurysm wall; their production and degradation depend on the stretch of the wall and are responsible for aneurysm growth. Biochemical and molecular studies have supported this hypothesized association between estrogen and formation, rupture of cerebral aneurysm. The collagen wasting commonly observed in bone and skin in the postmenopausal period due to decreased estrogen levels could possibly be responsible for the formation of aneurysms in the proximal segments of the cerebral arteries, as it occurs in various connective tissue diseases. Estrogen has been shown to scavenge reactive oxygen species following endothelial injury and also to inhibit their formation. Tightly regulated proteolytic degradation of the extracellular matrix is an important component of normal vascular homeostasis but, if poorly controlled, it may contribute to the pathogenesis of cerebral aneurysms. Of particular interest is matrix metalloproteinase-2 which degrades type IV collagen and has been found to be elevated both in the serum of patients with cerebral aneurysms and within aneurysmal vessel wall tissue [4,5,7,12,14,26,34]. Estrogen has been found to improve lipid profiles and thus may reduce the risk for arteriosclerosis, which has been considered a risk factor for aneurysm formation because of altered hemodynamics [21]. While this may appear to directly contradict the aforementioned protective role of estrogen in maintaining vascular wall integrity, many regulatory mechanisms exist that explain and further support the advantage of premenopausal women.
Postmenopausal women with ever use of HRT also showed a reduced risk compared with postmenopausal women who had never used HRT. The putative role of estrogen in these epidemiologic findings is further supported by the finding that HRT seems to reduce the risk of SAH in postmenopausal women, possibly via the effects of estrogen on blood vessel walls, inflammation and homeostasis of the vascular wall matrix. However, the negative results for beneficial effects of HRT have been reported in several reports for menopausal symptoms. There is increasing evidence that the timing of HRT initiation may play a crucial role in determining chronic heart disease risk among estrogen users. And, significant drawback is that long-term HRT may increase the risk of breast cancer and meningioma in women [1,7,9,13,17,21,24,35].
There are some limitations to our study design. The first limitation relates to a relatively small number of cases (40 cases) is not sufficient to definitively conclude the effect of estrogen on formation, growth and rupture of cerebral aneurysm. Second, our study with age-matched found a meaningful trend between early menopause with lower estrogen hormone level and the formation of cerebral aneurysm and SAH. Despite showing group of an overall mean age at premenopause, had a smaller proportion of women in the general public, our results suggested that loss of estrogen earlier in a woman’s life may contribute to the pathogenesis of formation and rupture of cerebral aneurysm. Third, there are several well-known confounders, some of which are difficult to control and may confound the assessment of hormonal effect of cerebral aneurysms. They include the clinical conditions such as hypertension, diabetes mellitus, smoke and alcohol. For example, the factor of hypertension and smoke did significantly modify effect of hormonal factors. Being premenopausal had stronger negative association among women without a history of hypertension than among those with a history of hypertension. The reduced risk associated with being premenopausal was also much greater among those who had never smoked than among those who had smoked.
CONCLUSION
There is growing interest in the pathogenesis of cerebral aneurysm focused on the development of therapies to decrease the incidence of aneurysm growth and rupture. Estrogen deficiency in postmenopausal women has a significant impact on the pathophysiology of cerebral aneurysm and SAH. In our study, there is a trend showing that an earlier age at menopause related to estrogen hormone is associated with the aneurysmal SAH. Future study with large cases, well controlled and randomized is necessary to better understand the role of estrogen in cerebral aneurysm in humans in order to identify potential pathways for clinicians to target for intervention to prevent or treat the cascade of events that produce aneurysmal SAH.
Notes
No potential conflict of interest relevant to this article was reported.