How Subsidence Affects Clinical and Radiological Outcomes after Stand-Alone Anterior Cervical Discectomy and Fusion on Patients with Degenerative Cervical Disease? A Long-Term Follow-Up Study
Article information
Abstract
Objective
We aimed to examine the long-term radiological and clinical outcomes after stand-alone anterior cervical discectomy and fusion (ACDF).
Methods
In total, we enrolled 20 patients and 31 treated segments with degenerative cervical disease that underwent stand-alone ACDF with ≥60months of follow-up. Segmental angle (SA), cervical sagittal alignment (CSA), subsidence, and fusion were evaluated. A visual analogue scale (VAS) and the neck disability index (NDI) were applied pre- and post-operatively and at the last follow-up.
Results
Subsidence occurred in 9 (45%) patients and 15 segments (48.4%) at the last follow-up. The mean VAS and NDI scores had improved in both groups with and without subsidence. The mean SA at the last follow-up had significantly increased to 2.3°±8.5° in the subsidence group and to 1.7°±5.2° degree in the non-subsidence group compared to the post-operative SA (p<0.001). The overall mean CSA at the last follow-up significantly increased overtime in both groups from the postoperative CSA (p=0.003). The fusion rate was 86.7% in the subsidence group and 81.3% in non-subsidence group. However, the difference in SA, CSA and fusion rates between the two groups were not statistically significant (p=0.119, 0.98, and 0.682, respectively).
Conclusion
As a result of a long-term follow-up study after stand-alone ACDF, subsidence occurs to some extent. Still, it does not appear to significantly impact radiological and clinical outcomes if the clinician performs sufficient decompression of foramen during surgery. Subsidence seems to have a positive influence on the fusion rate.
INTRODUCTION
Anterior cervical discectomy and fusion (ACDF) with plate fixation has been recommended for degenerative cervical disease of two or more levels, with instability and kyphosis15,25). However, adding a cervical plate is associated with plate-related complications such as material failure, dysphagia, and adjacent segment degeneration (ASD)13,17). For these reasons, recent studies suggest that stand-alone ACDF without plate fixation is a safe and effective treatment option for cervical degenerative disease16,18). These reports, however, had a follow-up period of two years or fewer. Additionally, the most important issue of stand-alone ACDF is cage subsidence, which can cause kyphotic segmental change or kyphotic recurrence. As per some studies, cage subsidence is reported to have occurred in 19.1% to 62.5% of the patients who underwent stand-alone ACDF1,2,5,22,23). Some studies reported that stand-alone ACDF is not satisfactory with worse radiologic outcomes than ACDF with plate fixation10,11). Nevertheless, cage subsidence and segmental kyphotic change were not significantly associated with clinical outcomes in a short follow-up period7,8).
The objective of this study was to evaluate the feasibility of standalone ACDF using polyether ether ketone (PEEK) cages without plate fixation by analyzing the long-term clinical and radiological outcomes.
MATERIALS AND METHODS
1. Patient Population and Study Design
We conducted a retrospective review of 304 patients with degenerative cervical disease who underwent ACDF with or without plate fixation between 2005 and October 2015 at our institution. The inclusion criteria were as follows: (1) patients with signs and symptoms of cervical radiculopathy or cervical spondylotic myelopathy who were unresponsive to medical treatment, (2) patients treated with one-, two-, or multiple level stand-alone ACDF, and (3) clinical and radiologic follow-up of ≥60 months after surgery. The exclusion criteria were as follows: (1) patients who underwent previous cervical spine surgery, (2) patients with other cervical disease including infection or tumor, and (3) patients with <60 months clinical or radiological follow-up after surgery.
In total, we enrolled 20 study patients with degenerative cervical disease who underwent stand-alone ACDF with ≥60 months follow-up. To identify the patients’ clinical characteristics, clinical data at the time of treatment, including age, sex, presenting symptoms, bone mineral density, level of surgery, plain radiographs, computed tomography (CT) scans, and magnetic resonance imaging scans of the cervical spine were collected.
2. Surgical Technique
General anesthesia was used in all patients. Standard Smith-Robinson method was performed to expose the involved segment. The proper PEEK cage was selected (Solis® cage, Stryker Spine, Allendale, NJ, USA; Cornerstone cage, Medtronic, Memphis, TN, USA). The cages were packed with a demineralized bone matrix (SureFuseTM; Hansbiomed Corp., Seoul, Korea), mixed with autologous bone chips, and inserted into the disc space. The operation was completed without anterior plating.
3. Radiological and Clinical Evaluation
CT was performed at 6 months after surgery and once a year thereafter to evaluate fusion. Fusion was defined as less than 2-mm motion between the spinous processes on flexion-extension lateral radiographs, less than 50% of radiolucency covering the implant’s outer surface, and the presence of continuous bridging trabeculae at the graft on simple lateral radiographs or CT scans21). The cervical sagittal alignment (CSA), segmental angle (SA), and subsidence were measured using lateral plain radiographs. The overall CSA was measured according to the Cobb’s angle (CA) between the lower endplate of C2 and the lower endplate of C7. SA was also measured using the CA, the angle between the superior endplate of the upper adjacent vertebra, and the inferior endplate of the lower adjacent vertebra at the operated disc level. Kyphosis was noted as a positive value, while lordosis was noted as a negative value. Subsidence was defined as a decrease in the total intervertebral height (TIH) between the two adjacent vertebral bodies on comparing post-operative lateral plain radiographs. The TIH was measured at three points: anterior, middle, and posterior points of the superior endplate of the upper adjacent vertebra and the inferior endplate of the lower adjacent vertebra at the operated disc level (Fig. 1). Based on serial TIH analysis, subsidence was defined if the TIH decreased more than 3.0mm at any three points than the TIH taken post-operatively5,6,10).

Cervical sagittal alignment (CSA), segmental angle (SA), anterior intervertebral height (AIH), middle intervertebral height (MIH), and posterior intervertebral height (PIH) on lateral radiographs of cervical spine.
To evaluate pain in the neck and arms, a visual analogue scale (VAS) was applied pre- and post-operatively. Additionally, the neck disability index (NDI) questionnaire was administered pre- and postoperatively and at the last follow-up.
4. Statistical Analysis
The data of this study were entered into SPSS version 25.0 (SPSS Inc., Chicago, IL USA), and χ2 test was used to compare the qualitative data between the groups. The one-way ANOVA test was used for quantitative data. Paired samples t-test was used to evaluate the results before and after surgery. The independent t-test and Mann-Whitney U test for parametric or nonparametric variables were used for analyzing relationships between clinical and radiologic results and subsidence. Quantitative data were presented as the mean and standard deviation and qualitative data were presented as frequency or percentage. A p-value of less than 0.05 was considered as a significant relationship.
RESULTS
1. Patient Characteristics
A total of 20 patients with a total of 31 treated segments were included in this study. The mean age of the patients at the time of stand-alone ACDF was 59 years (range, 30–74 years). There were 16 (80%) male patients and 4 (20%) female patients. The number of stand-alone ACDF procedures at one-, two-, and three-segments was reported in 10 (50%), 9 (45%), and 1 (5%) patient, respectively. Stand-alone ACDF was commonly performed at the C5–6 level (14 segments, 45.2%), followed by C6–7 level (9 segments, 29.0%), C4–5 level (5 segments, 16.1%), and C3–4 level (3 segments, 9.7%). The overall mean follow-up period after surgery was 77 months (range, 60–150 months). The clinical characteristics of the enrolled patients are summarized in Table 1.

Clinical characteristics of patients
2. Radiological Outcomes
Fusion was achieved in 26 segments (83.9%) at the last follow-up. Subsidence occurred in 9 (45%) patients and 15 segments (48.4%) at the last follow-up. The patients were divided into the subsidence group and non-subsidence group. In the subsidence group, there were 8 male and 1 female patient with a mean age of 55.3 years (range, 31–74 years). In the non-subsidence group, 8 male and 3 female patients with a mean age of 47.9 (range, 30–71 years). The mean follow-up duration was 68.5months (range, 60–96 months) and 85.8 months (range, 60–150 months) in the subsidence group and non-subsidence group, respectively (Table 2). The decrease in intervertebral height mainly occurred on the anterior, middle, and posterior portions at the same time. Anterior-only, middle-only subsidence, and combined anterior and middle subsidence occurred; however, posterior-only subsidence was not observed. The mean anterior intervertebral height (AIH), middle intervertebral height (MIH), and posterior intervertebral height (PIH) in the subsidence group decreased by 6.1±2.5, 6.0±2.8, and 4.6±3.1mm, respectively, and in non-subsidence group, they decreased by 1.5±1.3, 1.5±1.2, and 1.2±1.4mm, respectively, from the values recorded immediately after surgery to those recorded at the last follow-up. Although the AIH, MIH, and PIH significantly decreased from after surgery to the last follow-up in both groups, TIH significantly decreased more over time in the subsidence group than in the non-subsidence group (p<0.0001). The AIH, MIH, and PIH had mostly changed within one-year after surgery (Fig. 2). The overall mean SA of the last follow-up significantly increased by 2.3±8.5 degree at the last follow-up in subsidence group and 1.7±5.2 degrees in the non-subsidence group compared to the values postoperatively (p<0.001), but there was no significant difference between the two groups (p=0.119). The overall mean CSA at the last follow-up significantly increased overtime in both groups compared with that reported post-operatively (p<0.001); the difference between the two groups was not statistically significant (p=0.98). The fusion rate at the last follow-up was 86.7% in the subsidence group (13 of 15 segments) and 81.3% in non-subsidence group (13 of 16 segments) in segmental analysis, and the difference in the fusion rates between the two groups was not statistically significant (p=0.682) (Table 3). Regarding the non-fusion levels in both groups, there were no worsening of clinical symptoms and radiological findings, additional surgical treatment was not necessary throughout the follow-up period.
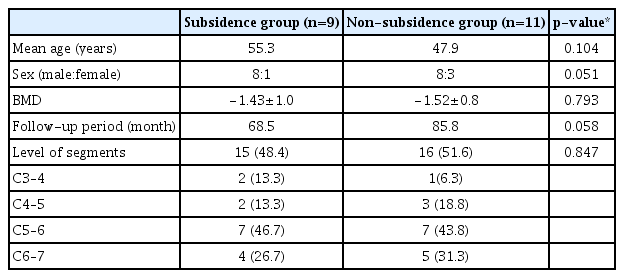
Patients’ characteristics of subsidence and non-subsidence group

(A–C) Changes in anterior intervertebral height (AIH), middle intervertebral height (MIH), and posterior intervertebral height (PIH) preoperative, immediate post-operative, 1 year, and 2 years post-operatively, and at the last follow-up between subsidence and non-subsidence group.
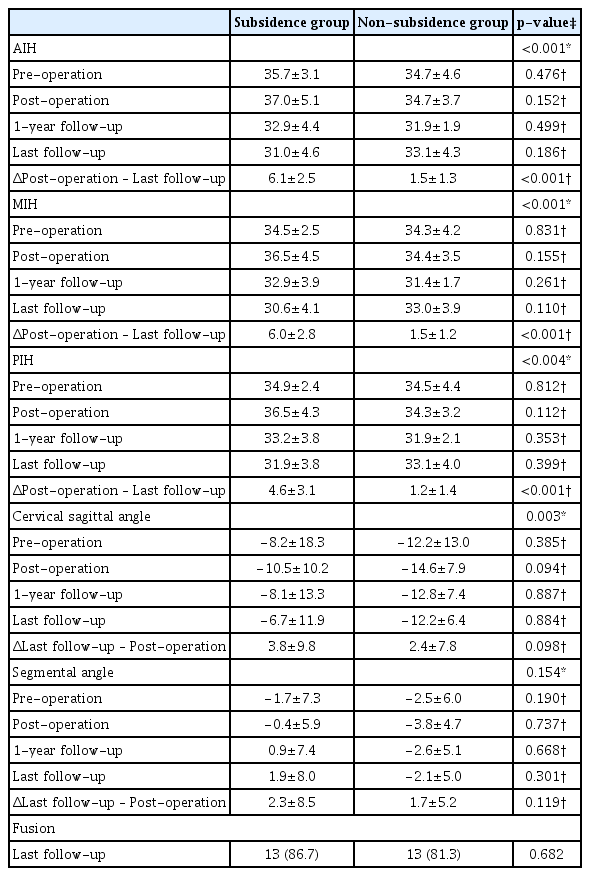
Radiological outcomes
3. Clinical Outcomes
The overall pre-operative VAS score of neck pain was 3.1±2.2 and 3.0±1.0 at the last follow-up. At the last follow-up, the score had significantly improved to 3.5±2.2 and 4.1±1.1 in the subsidence group and non-subsidence group, respectively (p<0.001); and there was no statistical difference between the two groups (p=0.441). The overall pre-operative VAS score of arm pain was 3.9±1.8 and 3.3±1.8 at the last follow-up. At the last follow-up, it had significantly improved to 3.3±1.7 and 3.6±1.4 in the subsidence group and non-subsidence group, respectively (p<0.001); and there was no statistical difference between the two groups (p=0.632). Furthermore, the NDI score had improved over time during the follow-up period in both groups (p<0.001), and the difference was not statistically significant (p=0.706) (Table 4). No patients reported worsening pain or an increase in the NDI score during the follow-up period.
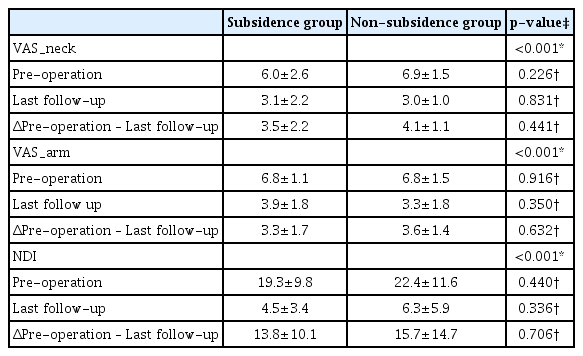
Clinical outcomes
DISCUSSION
ACDF with plate fixation has been considered the “gold standard” for safe and solid cervical interbody fusion in the treatment of degenerative cervical disease15,25). Anterior plate fixation improves cervical spine stability, enhances the fusion rate, and maintains the intervertebral height and cervical physiological curvature, thus reducing the complications of post-operative graft collapse and loss of physiological curvature12). In addition, various materials have been developed and used for interbody grafts with the ACDF, in order to avoid morbidity associated with autologous bone grafts. PEEK material cages have been developed to achieve immediate stability and successful bone fusion3). With the development of synthetic cages and bone-inductive substances, questions have arisen about the need for additional anterior plate fixation which can lead to complications such as material failure, dysphagia, and ASD13,14,17,19). Recently, several studies suggested that stand-alone ACDF is a safe and effective modality for cervical degenerative disease4,16,18,20,24). However, it remains controversial because the outcome of the standalone ACDF of these reports included only two-year or much lower follow-up periods. In this study, we revealed a radiological and clinical long-term outcome with a follow-up period of more than 5 years after stand-alone ACDF.
The main consideration relating to stand-alone ACDF is subsidence. The generally accepted hypothesis regarding subsidence after standalone ACDF is that, since there is no plate to support axial loading, the intervertebral space collapses as the implant penetrates the vertebral body. Kim et al.10) reported that the subsidence occurred 58.6% after performing stand-alone ACDF with an average 5-year follow-up. They suggested that the subsidence was progressed over time continuously until the last follow-up period. In addition, the VAS score of the patients’ neck and arm increased, the patient’s satisfaction was assessed using Odom’s criteria, and 64.6% of patients responded as unsatisfactory at the last follow-up. However, no statistical association was found between subsidence and clinical outcome. In our study, although the 48.4% subsidence occurred, neck and arm pain were relieved, and NDI scores improved at the last follow-up (p<0.001). None of the patients experienced worsening pain or neurologic symptoms after surgery, and no clinically negative outcomes associated with subsidence were reported. In addition, the decrease of intervertebral height mostly occurred within one-year after surgery, after that, we could find the tendency of decrease of intervertebral height was negligible until the last follow-up in non-subsidence group (Fig. 2). Similarly to our results, many previous reports revealed that the subsidence was not significantly associated with clinical outcome, and mostly occurred within one-year after surgery and then be stabled7–9,11). If the subsidence occurs, it may be assumed that the foraminal height would also decrease, affecting clinical outcomes. However, the VAS score of arm pain in subsidence group was significantly improved (p<0.001) in our study. We suggest that if foramen decompression is adequately and sufficiently performed during surgery, subsidence does not affect the clinical outcome.
The fusion rate reached 82.8% with good stability in our study. With the development of synthetic cages and bone-inductive substances, the use of anterior plating in ACDF did not seems to provide obviously high fusion rates. Meanwhile, Wu et al.23) reported that rigid anterior plating may act as a shield for the mechanical load, which is very important for fusion. It has been hypothesized that during the process of bone fusion and remodeling, cage subsidence could be the consequence of cage settlement, contributing to mechanical loading of the bone graft inside the cage, thus promoting fusion2,22). Many reports have revealed that stand-alone ACDF achieved a successful fusion rate higher than 90%4,18,20). Although not statistically significant, our study showed higher fusion rates in the subsidence group than in the non-subsidence group (Table 3). Regrading cervical stability, although the changes in CSA and SA values from the post-operative to the last follow-up values were larger in subsidence group than in the non-subsidence group, the difference between the two groups was not statistically significant. Considering that the pre-operative CSA and SA values in the sub-sidence group were larger than those in the non-subsidence group, it can be assumed that the pre-operative CSA and SA values may affect the amount of change in the post-operative CSA and SA values. Consequently, stand-alone ACDF does not seem to be the only factor in the deterioration of SA and CSA.
Except for subsidence, no surgery-related complications occurred. In addition, although subsidence had occurred in 48.4% of the patients, their VAS or NDI scores had improved and additional surgical treatment was not necessary throughout the follow-up period. In addition, until now, most previous reports have failed to explain the subsidence as a factor predicting low fusion rates, unsatisfactory clinical outcomes, and kyphotic change after surgery7,8). Subsidence is an inevitable consequence of stand-alone ACDF; we suggest that proper subsidence with the sinking of cages into the vertebral bodies may contribute to solid fusion and does not adversely affecting clinical outcomes and cervical alignment.
This retrospective study had some limitations. This study comprised a small number of patients, and there was no control group to compare the radiological and clinical outcomes. Moreover, the predictive factors for subsidence and kyphotic change were not determined. Further randomized prospective studies are needed to determine the efficacy and toxicity associated with stand-alone ACDF surgery.
CONCLUSION
As a result of a long-term follow-up study after stand-alone ACDF, subsidence occurs to some extent. Still, it does not appear to significantly impact radiological and clinical outcomes if the clinician performs sufficient decompression of foramen during surgery. Subsidence seems to have a positive influence on the fusion rate. Overall, stand-alone ACDF appears to be an acceptable surgical option for treating degenerative cervical disease.
Notes
No potential conflict of interest relevant to this article was reported.