Spontaneous Resorption of Lumbar Disc Herniation with Literature Review: Caution before Deciding on Surgery
Article information
Abstract
Lumbar disc herniation (LDH) is a common cause of sciatica. Several cases of clinical improvement in patients with spontaneous resorption of LDH have been reported. However, it is uncommon for this spontaneous resorption of LDH to manifest as an abrupt improvement of symptoms. Here, we report a case of rapid symptom improvement due to spontaneous resorption of LDH. Furthermore, we review the available literature to critically evaluate the possibility of spontaneous LDH resorption and consequent symptom improvement within the context of previous research.
INTRODUCTION
Sciatica due to lumbar disc herniation (LDH) occurs in 0.1% to 0.5% of adults every year16). The most severe form of LDH is a sequestered disc, in which the sequestration, also called a free fragment, is no longer attached to each intervertebral disc2). Although surgery is generally known to be effective for treating LDH, several studies6,7) have noted that the majority of LDH cases could improve with conservative treatment. Here, we report a case in which symptoms were dramatically improved by sequestrated disc resorption.
CASE REPORT
In September 2019, a 35-year-old male patient visited our hospital with pain in both lower extremities (visual analog scale [VAS]9). The patient underwent 6 months of conservative treatment at other hospitals. However, treatment was unsuccessful, and he was admitted to our outpatient clinic. Magnetic resonance imaging (MRI), performed at another hospital in March 2019, revealed that the 4th to 5th lumbar disc showed a correlation between disc position and pain in both extremities; therefore, surgery was recommended (Fig.1). One week later, during preoperative hospitalization, the pain had improved (VAS 3); the patient was asked to undergo additional imaging tests, but he refused and requested surgery. Thereafter, laminectomy and ligament removal surgery were performed according to the MRI image. No sequestrated disc material was identified during the operation, and no specific changes were observed after the operation. After surgery, computed tomography (CT) was performed instead of MRI, due to the patient’s financial constraints. A comparison with the previous MRI confirmed that there was significant disc material resorption (Fig.2). The patient was discharged 3 days after surgery with the improvement of symptoms and no complications. The observation was continued without additional treatment, and the patient's condition remained good until 24 months after surgery.
(A, B) Sagittal and (C, D) axial preoperative T2-weighted magnetic resonance images of the 35-year-old male patient reveal a large disc extrusion and severe dural sac compression, center to left, at the L4-5 level.
(A, B) Sagittal and (C, D) axial postoperative computed tomography demonstrate that the disc fragments were resorbed, with a residual small disc protrusion at the L4-5 level.
DISCUSSION
LDH is a common disorder that limits patients’ functional ability, leading to disability and reduced quality of life. Several studies have observed that the reuptake of LDH occurs via a phagocytic mechanism involving macrophages, triggering an inflammatory response and angiogenesis in the outermost layer of the prolapsed disc material3,11). In addition, the degradation of proteoglycans in the nucleus pulposus leads to dehydration of the prolapsed disc material, reducing disc volume4,12). Apoptosis may further influence disc resorption9,10).
In this case, clinical symptoms improved rapidly after 6 months and dramatic disc resorption was confirmed by imaging studies performed during follow-up. Many prior studies have reported the occurrence of spontaneous resorption in the conservative treatment of herniated discs. Ahn et al.1) showed that 67% of LDH cases showed dramatic resorption after an average follow-up period of 4.3 months. In addition, Benson et al.5) found that 83% (29/35) of patients with massive LDH showed complete and sustained recovery with an average follow-up period of 23.2 months. In other studies, the majority of patients who underwent non-surgical treatment showed improvement in clinical and imaging follow-up (Table 1)4,8,14). A meta-analysis of 11 studies by Zhong et al.20) showed that the overall incidence of spontaneous absorption after LDH was 66.66% (95% confidence interval, 55.12–78.21).
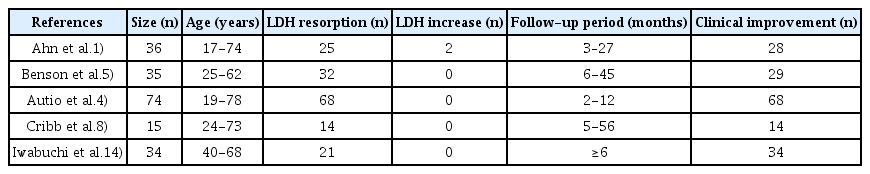
Changes in LDH and other characteristics reported in studies of non-surgical treatment
However, several studies have reported an increase in LDH following conservative treatment6,18). Large LDHs tend to degenerate more easily than small LDHs. During infiltration of the annulus fibrosus or posterior longitudinal ligament, the disc material is exposed to the systemic circulation within the epidural space, thereby enhancing cell-mediated inflammatory responses. Larger discs are more likely to shrink in size than smaller discs, while smaller discs can potentially increase in size17).
The patient in this case study showed rapid symptom improvement. Accordingly, we sought to better understand the relationship between the degree of LDH resorption and the extent of symptom improvement. Seo et al. suggested that clinical outcomes improved extensively in patients with a decrease in LDH volume19). However, other studies have suggested that chemical factors influencing the pathophysiology of sciatica may play a role13,15). In our patient, the LDH volume decreased for six months after the MRI performed in March 2019. However, sudden symptom improvement was noted, regardless of the decrease in LDH volume.
Therefore, even if the patient's symptoms improve suddenly, this improvement may be temporary, and an imaging test, such as an MRI or CT, should be performed to confirm the LDH volume right before surgery. However, the patient in this case study was unfortunately unable to undergo MRI before and after surgery, as this is not covered by Korea's insurance policy, and the cost burden was too high for the patient to fund himself.
CONCLUSION
In this report, we described a case of sequestrated disc resorption and the subsequent abrupt clinical improvement. Since LDH is well absorbed and symptoms have been observed to improve spontaneously in some cases, and many cases respond well to conservative treatment, it is necessary to verify the LDH volume just before surgery. Further, if 6 months have passed between the initial imaging and the operation, or if changes to the clinical symptoms occur, an imaging follow-up examination such as an MRI is absolutely necessary.
Notes
No potential conflict of interest relevant to this article was reported.
Ethical approval and patient consent: The study protocol was approved by the Institutional Review Board of Asan Medical Center (IRB no. 2022-0145).