Characteristics of Cervical Spine Injuries Caused by Industrial Accidents: The Experience of a Single Regional Trauma Center in South Korea
Article information
Abstract
Objective
This study examined the characteristics of patients with cervical spine injuries caused by industrial accidents and analyzed the factors related to mortality.
Methods
: In total, 424 patients with cervical spine injuries who visited our hospital from 2016 to 2020 were divided into an industrial accident and non-industrial accident groups. Age, sex, fracture severity, facet injury, high cervical injury, spinal epidural hematoma, spinal cord injury, shock, arrival route, Injury Severity Score (ISS), Glasgow Coma Scale (GCS), mortality, and trauma mechanism were compared between the two groups. Regression analysis was performed to determine the factors affecting mortality.
Results
Industrial accident patients significantly differed from the rest of the study population in terms of the sex ratio (male ratio, 95.1% vs. 77.8%; p<0.001), arrival route (direct transport, 61.2% vs. 50.9%; p=0.017), and trauma mechanism (p<0.001). Among the trauma mechanisms, falls had the largest difference between industrial accident patients and all patients (55.3% and 28.1%, respectively). Significant associations with mortality were found for falls (odds ratio [OR], 22.330; p=0.015), ISS (OR, 1.056; p=0.008), GCS <9 (OR, 0.014; p<0.001), and shock (OR, 7.290; p<0.001).
Conclusion
Falls were the most frequent trauma mechanism of cervical spine injuries in patients who experienced industrial accidents. The factors significantly correlated with mortality were falls, ISS, GCS <9, and shock.
INTRODUCTION
Cervical spine injuries are not typically accompanied by other injuries, compared to thoracolumbar spinal injuries18). Therefore, it is relatively easy to isolate and evaluate the impact of cervical spine injuries on the patient's prognosis as the impact of injuries in other organs is minimal27). Due to the highly mobile nature of the cervical spine, serious injuries, such as spinal cord injuries, can occur even with low-energy forces that do not cause fractures14,27). Despite a small degree of damage, upper spinal cord injury due to cervical spine injury can significantly affect the neurological symptoms and functional prognosis of the patient across the whole body.
The prevalence of spine injury and accompanying spinal cord injury differs across countries and regions6,28). In the case of spinal cord injury, in developed nations, it has been reported variably as 11.5 to 53.4 persons per million persons and 13.0 to 220.0 persons per million2,7,17,23).
There have been limited investigations on the prevalence of spinal injuries in South Korea. Despite the limited studies on spinal cord injury, those using the Health Insurance Review and Assessment Service data have recently been reported, but patients in industrial and traffic accidents were not included5).
Our trauma center is near petrochemical and heavy industry complexes such as oil refineries and large shipyards, so we manage patients from various industrial accidents. In addition, cervical trauma caused by industrial accidents is estimated to have poor outcomes due to the severity of the trauma mechanism.
Therefore, this is the study to examine the characteristics of patients with cervical spine injuries caused by industrial accidents and analyze the factors related to mortality.
MATERIALS AND METHODS
This study was approved by our Institutional Review Board, and the requirement for informed consent was waived due to the retrospective nature of this study. (2021-04-039)
This retrospective, the single-centered study enrolled 45,586 patients who visited our emergency room due to trauma from January 2016 to May 2020. Among them, 424 patients with cervical spine injuries were included. Patients with cervical spine injury patients were classified as industrial accident patients (n=103) and the total patients (n=424). Industrial accident patients were defined as patients who had injuries that occurred during work hours according to the emergency room medical record review. For each patient group, age, sex, fracture severity, facet injury, high cervical injury, spinal cord injury, level of spinal injury, spinal epidural hematoma, traumatic brain injury (TBI), trauma mechanism, Injury Severity Score (ISS), Glasgow Coma Scale (GCS), shock, visit route, hospital stay, intensive care unit stay, and mortality were analyzed. Trauma mechanisms were classified as driver traffic accidents (TAs), passenger TA, pedestrian TA, motorcycle accidents, bicycle accidents, falls, slips, heavy equipment accidents, and others.
The fracture severity was classified into grade 0 to 3 as indicated by the AO Spine Subaxial Cervical Spine Injury classification system25) (Grade 0: No fracture or AO spine subaxial classification A0; Grade 1: AO spine upper cervical classification type A, AO spine subaxial classification A1 to A4; Grade 2: AO spine upper cervical classification type B, AO spine subaxial classification type B; Grade 3: AO spine upper cervical classification type C, AO spine subaxial classification type C). The injury level was divided into upper (C2 or higher) and lower cervical spine (C3 or lower). The shock was a systolic blood pressure of <90 mmHg in the emergency room. Facet injury, spinal cord injury, spinal epidural hematoma, TBI, and mortality were classified as present or absent.
Statistical Analysis
The SPSS software (version 24.0; IBM Corp., Armonk, NY, USA) was used for statistical analysis. Categorical variables were analyzed by performing the chi-square test, while continuous variables were by performing the independent sample t-test. In addition, multiple regression analysis was performed to confirm the relationship between each factor on mortality.
RESULTS
Of the 424 patients with cervical spine injuries, when comparing total patients and industrial accident patients, 330 (77.8%) and 98 (95.1%) were men. The male ratio was significantly higher in the industrial accident patients compared to the total patients (p<0.001). The mean age for the total and industry accident patients was 53.58 ± 15.91 and 53.94 ± 13.36, respectively, with no significant difference. There were no significant differences in fracture severity, facet injury, high cervical injury, spinal epidural hematoma, spinal cord injury, ISS, GCS, shock, TBI, hospital stay, and intensive care unit stay.
When compared based on the visit route, there was a significant difference in direct transport with 216 (50.9%) in the total patients and 63 (61.2%) in the industrial accident patients (p=0.017). There was also a significant difference in the trauma mechanisms (p<0.001). For the total patients, there were 70 driver TAs (16.5%), 42 passenger TAs (9.9%), 48 pedestrian TAs (11.3%), 35 motorcycle TAs (8.3%), 32 bicycle TAs (7.5%), 119 incidents of fall (28.1%), 45 slips (10.6%), 8 heavy equipment accidents (1.9%), and others were 25 (5.9%). Meanwhile, for the industrial accident patients, the incidence of driver TA was 14 (13.6%), passenger TA was 1 (1.0%), pedestrian TA was 2 (1.9%), motorcycle TA was 1 (1.0%), bicycle TA was 0 (0.0%), fall was 57 (55.3%), slip was 5 (4.9%), heavy equipment accident was 8 (7.8%), and others were 15 (14.6%). Among the trauma mechanisms, there was a marked difference between the total patients and the industrial accident patients in the category of falls (Table 1).

Comparison of all patients and industrial accident patients with cervical spine injuries
Simple and multiple regression analyses were performed for each factor to elucidate the contributing factors of mortality in patients with cervical spine injuries.
In simple regression analysis, high cervical injury (p<0.001), spinal cord injury (p=0.002), ISS (p<0.001), GCS <9 (p<0.001), shock (p<0.001), and TBI (p<0.001) were statistically significant. In multiple regression analysis, fall injury mechanism (p=0.015; odds ratio [OR], 22.330; 1.812-275.180), ISS (p=0.008; OR, 1.056; 1.015-1.099), GCS <9 (p<0.001; OR, 0.014; 0.003-0.065), and shock (p=0.001; OR, 7.290; 2.182-24.349) were statistically significant (Table 2).
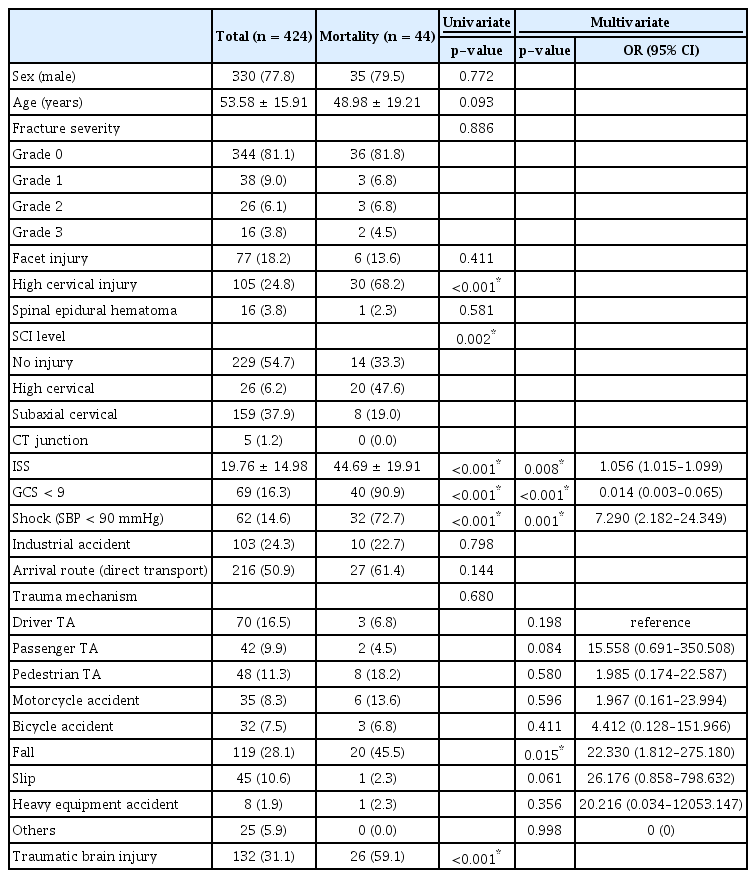
Contributing factors to mortality in patients with cervical spine injury
The frequency of the anterior, posterior, and anteroposterior fusions was compared in patients who underwent fusion due to cervical spine injury, depending on whether they were industrially or non-industrially injured. For 74 patients with a non-industrial accident, anterior fusion was performed in 42 patients (56.8%), posterior fusion in 22 (29.7%), and anteroposterior fusion in 10 (13.5%). Furthermore. 10 (50.0%) out of 20 patients who had industrial accidents underwent anterior fusion, posterior fusion in 3 (15.0%), and anteroposterior fusion in 7 (35.0%). Moreover, the proportion of industrial accident patients who underwent anteroposterior fusion was higher than that of non-industrial accident patients, but there was no statistically significant result (p=0.066). The number of fusion segments was compared to whether the patient had an industrial or a non-industrial accident and underwent fusion due to cervical spine injury. In the case of non-industrial accident patients, 1- (n=21, 28.4%), 2- (n=35, 47.3%), 3- (n=11, 14.9%), and 4-segment fusions (n=7, 9.5%) were implemented. In addition, in the case of industrial injury patients, 1- (n=11, 55.0%), 2- (n=5, 25%), 3- (n=1, 5%), and 4- (n=3, 15.0%) were implemented. There was no clear difference between the two groups and no statistical significance was observed (p=0.080). In the industrial accident patient group, whether the operation with spinal fusion was investigated based on the fall mechanism. Finally, in the non-fall group (n=46), fusion was performed in 5 patients (10.9%), while in the fall patient group (n=57), fusion was performed in 15 patients (26.3%). The difference between the two groups was statistically significant (p=0.049) (Table 3).
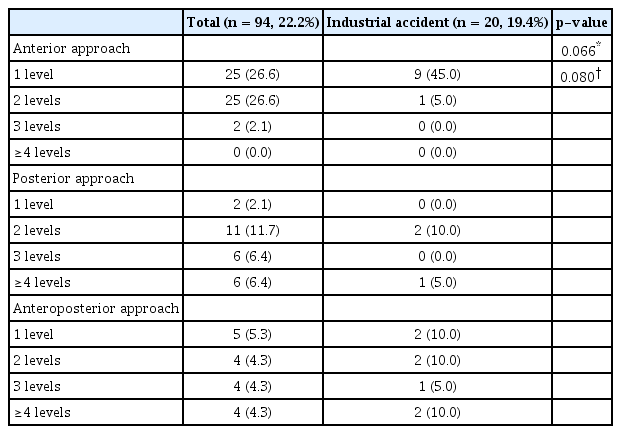
The operation type and the number of segments of spinal fusion in patients with industrial accidents
DISCUSSION
The ratio of men, direct transport, and fall trauma mechanism was higher in industrial accident patients than in the total patients. Regarding sex, the ratio of male workers tends to be high because our trauma center is located in heavy industry and chemical complexes. The direct transport rate is high in industrial accident patients because the patient transfer system is relatively capable in case of an accident in the workplace. In addition, it is considered that the falling ratio is high because there are many high-altitude work sites due to the nature of heavy industry work, such as shipyards1).
Mortality was associated with ISS, GCS, and shock8,13). In the case of high cervical injury and TBI, the univariate analysis showed a significant correlation, but the multivariate analysis did not. This may be due to the confounding effect of falls, which is significantly related to the trauma mechanism15). For the trauma mechanism, it was confirmed that TBI (p=0.006, coefficient 0.137) and high cervical injury (p=0.005, coefficient 0.136) had a significant correlation from the Pearson correlation analysis results. This is due to the high energy mechanism of a fall, which has a high rate in the trauma mechanism of industrial accident patients.
As described above, it was confirmed that fall appears as a factor influencing mortality due to cervical spine injury, but its effect on mortality does not solely depend on its high energy mechanism. Falling from both high and low heights may cause spinal injuries4). Although not differentiated in this study, a fall from a relatively low height (approximately 1 m) can cause significant damage to the cervical spinal cord4). This is particularly significant for middle-aged and older populations with underlying cervical spondylosis5,19,20,22). In a study by Zhang et al.29) with 1,858 patients with traumatic spinal injury, a fall from a low height occurred more frequently with older age. The incidence of associated injuries to other body parts was low but had more severe neurologic deficits, suggesting cervical or upper thoracic cord injury29). As the population of industrial workers is aging, more attention should be given to preventing fall (high and low heights) injuries.
Although the prevention of accidents in industrial sites is very important, whenever a cervical cord injury occurs, a quick initial evaluation should be done, and when necessary, prompt intervention is required24). Fehlings et al.9) conducted a multicenter, nonrandomized, prospective cohort study comparing the differences in neurological prognosis depending on whether early surgery was performed in 313 patients with cervical cord injury and showed that patients who underwent early decompression surgery showed a significantly higher rate of >2-point grade improvement in the American Spinal Injury Association Impairment Scale 6 months after receiving the treatment than the group without early decompression surgery (OR, 2.83; 95% confidence interval, 1.10–7.28). Thus, it is necessary to transport patients directly to a trauma center that can promptly manage these patients after being dispatched from the scene. In this study, the direct transport rate of patients with cervical spine injury due to industrial accidents was approximately 61.2%, higher than the total patients (50.9%). Therefore, it is necessary to strengthen coordination between industries and emergency transport authorities to improve the direct transport rate to trauma centers.
In the analysis of patients who underwent spinal fusion for a cervical spine injury, the proportion of industrial accident patients who underwent simultaneous anteroposterior fusion compared to non-industrial accident patients tended to be higher but was not statistically significant. In the subgroup analysis of the operation with spinal fusion, the spinal fusion frequency was significantly higher in patients with injuries caused by a fall. This may be due to the degree of instability caused by high-energy injuries being relatively higher in industrial accident patients, especially those in the fall group. In this study, the AO spine subaxial cervical spine injury classification system was used as a classification criterion for the degree of cervical spine injury. However, in the Allen and Ferguson classification, which was based on the mechanism of cervical spine injury, the prognosis may be particularly poor in the distractive extension injury due to the accompanying spinal cord distraction and brain stem injuries11,26). This study introduced the cases of distractive extension injury among cervical spine injury patients (Fig. 1, 2).

Fatal cases of distractive extension injury–induced cervical dislocation. (A) A 58-year-old man was injured in a pedestrian traffic accident. Cardiopulmonary resuscitation (CPR) was performed during transport to the hospital. Cervical dislocation at C1/2 was confirmed, and no specific damage was confirmed in other body parts. He expired the day after admission. (B) A 55-year-old man was injured in a pedestrian traffic accident. CPR was performed on-site. Cervical dislocations at C1/2, C6/7 and traumatic subarachnoid hemorrhage were confirmed, and no other specific damage was confirmed in other body parts. He expired in the hospital on day 17 after admission. (C, D) A 60-year-old man was injured by falling from a 20-m height in a shipbuilding yard. CPR was performed while the patient was being transferred to our hospital after an initial evaluation at an external hospital. Cervical dislocations at C1/2 and C5/6 were confirmed, and emergency surgery was performed for thoracic and intra-abdominal bleeding. He expired on the third day of admission.
Surviving case of distractive extension injury–induced cervical dislocation. A 30-year-old man, wearing a helmet, had his upper body caught and damaged by heavy equipment. Cardiopulmonary resuscitation was performed on-site. Cervical dislocation at C2/3 was confirmed, and multiple rib fractures and pneumothorax were confirmed. Due to the patient’s poor general condition, surgical intervention for the cervical spine was performed on hospital day 35. He remained hospitalized for about a year due to treatment for bedsores and respiratory complications, and was then discharged with a tracheostomy using a portable ventilator. (A) Initial cervical spine X-ray. (B, C) Initial cervical spine computed tomography. (D) Sagittal plane of cervical spine magnetic resonance imaging. Brainstem signal intensity changes are confirmed. (E, F) Postoperative cervical spine X-ray.
Finally, when cervical spinal cord injury is suspected in the workplace, additional damage prevention is required through a cervical collar application. Patients with cervical spinal cord injury have limited functional recovery and a low rate of return to work after the injury10,12,16,21). Therefore when a cervical spinal cord injury is suspected, it is important to prevent further damage by applying preemptive cervical immobilization before transporting the patient3). In addition, educating field emergency personnel regarding these measures will improve patient outcomes. There are concerns about prophylactic cervical orthosis. In patients with reduced consciousness due to head injury, the cervical orthosis may cause an increase in intracranial pressure by inhibiting jugular venous return and may induce additional spinal cord injury by promoting cervical distraction in a cervical spine fracture accompanied by ankylosing spondylitis25). Therefore, caution is required in these circumstances.
This study has limitations. First, our study result may be biased due to its retrospective nature. Second, there was no direct association between industrial accidents and mortality. However, since the fall rate was high in patients with industrial accidents, and the trauma mechanism was significantly related to mortality, a relationship between industrial accidents and mortality may be assumed. Lastly, this study cannot represent all industrial accident patients. However, as our trauma center is the only tertiary general hospital and trauma center in the region that manages severe trauma patients, the characteristics of our industrial accident patients may be used as a reference.
However, as our trauma center is the only trauma center in the region that manages severe trauma patients, the characteristics of our industrial accident patients may be used as a reference. Third, in order to obtain accurate results, it is necessary to compare the non-industrial accident group and the industrial accident group directly. Although this study has a limitation in that the comparison between the total group and the industrial accident group is performed, it may be helpful to investigate the characteristics of the industrial accident group.
CONCLUSION
The most common mechanism of cervical spine injury in patients involved in industrial accidents is fall. Fall as the mechanism of injury, ISS, GCS <9, and shock had a significant correlation with mortality.
Notes
FUNDING
This research was supported by the Basic Science Research Program through the National Research Foundation of Korea (NRF) funded by the Ministry of Science and ICT (2019R1I1A3A0106356314).
No potential conflict of interest relevant to this article was reported.