Outcomes and Complications of Oblique Lateral Interbody Fusion as a Surgical Option in Elderly Patients (Over 70 Years Old) with Degenerative Spinal Disease
Article information
Abstract
Objective
As Korea has become a super-aging society, the number of elderly patients with degenerative spinal disease has steadily increased. This study aimed to evaluate the usefulness of oblique lumbar interbody fusion (OLIF) by comparing the results and complications between OLIF and open spinal fusion in elderly patients with degenerative spinal disease.
Methods
Thirty-one patients underwent one-level posterior lumbar interbody fusion (PLIF), and 35 patients underwent one-level indirect decompression OLIF. The clinical outcomes of the two patient groups were analyzed using the visual analog scale (VAS) and Oswestry Disability Index (ODI). Through a comparative analysis of pre- and post-operative images, we measured changes in disc height (DH) and foraminal height (FH), and investigated the occurrence of subsidence in each patient group. The cross-sectional area was measured using magnetic resonance imaging pre- and post-operatively in OLIF.
Results
The pre-operative VAS and ODI scores were similar between the two groups and tended to improve post-operatively. In the OLIF group, the estimated blood loss (EBL) was significantly lower, DH and FH gains were more frequent, DH and FH maintenance was better, and cage subsidence occurred less frequently. In OLIF, psoas paresis and approach-site hematoma occurred; however, all patients with psoas paresis recovered without further treatment before discharge. In the PLIF group, dural tears occurred in four patients who recovered without revision surgery.
Conclusion
OLIF enables indirect decompression, reduced EBL, shorter hospitalization, and lesser subsidence. OLIF is considered a beneficial, minimally invasive surgical method for elderly patients.
INTRODUCTION
According to the 2021 resident registration demographics of the Ministry of Public Administration and Security of the Republic of Korea, the number of people aged 70 years or older is approximately 5,060,00024). Korea has become a super-aging society, and the number of elderly patients with degenerative spinal diseases such as spinal stenosis, spondylolisthesis, and adult spinal deformities has been steadily increasing. Non-surgical treatments, such as physical therapy, medication, and injections, have been used as conservative treatment methods to improve the symptoms of elderly patients; however, many of those patients complain of persistent pain and functional impairment. Although elderly patients are reluctant to undergo surgical treatment, it should be considered in patients who do not respond effectively to conservative treatment. In spinal surgery for the elderly, the goals of treatment typically focus on alleviating pain, improving mobility, and restoring quality of life. Open spinal fusion can be dangerous in elderly patients because of relatively long skin incisions, extended anesthesia times, and extensive bleeding19). Therefore, open spinal fusion can be a burden for surgeons. One of the alternatives to this is oblique lumbar interbody fusion (OLIF), a minimally invasive surgery8,12,14). Our hospital has been steadily implementing OLIF in patients with degenerative spinal diseases since April 2018, and the patient group includes elderly patients aged >70 years. Therefore, this study aimed to determine whether OLIF is an appropriate surgical option for elderly patients with degenerative spinal diseases. This study aimed to evaluate the usefulness of OLIF by comparing its outcomes and complications with those of open spinal fusion in elderly patients with degenerative spinal diseases.
MATERIALS AND METHODS
1. Patient Selection
The 31 patients who underwent one-level posterior lumbar interbody fusion (PLIF) from April 2016 to October 2020, representing open spinal fusion, were included in the control group. This control group was retrospectively compared with 35 patients aged 70 who underwent one-level indirect decompression OLIF between February 2020 and April 2022. In both groups, bone mineral density, body mass index, and preoperative anesthesia were evaluated according to preoperative anesthesia evaluation based on the American Society of Anesthesiologists Classification. In addition, the patients’ underlying diseases and medical histories were investigated (Table 1). The study protocol was approved by the Institutional Review Board of Pusan National University Yangsan Hospital. Informed consent was not required because of the retrospective nature of this study. And this study approved by the Institutional Review Board (IRB) of Pusan National University Yang-san Hostpital (IRB No. 05-2023-080).
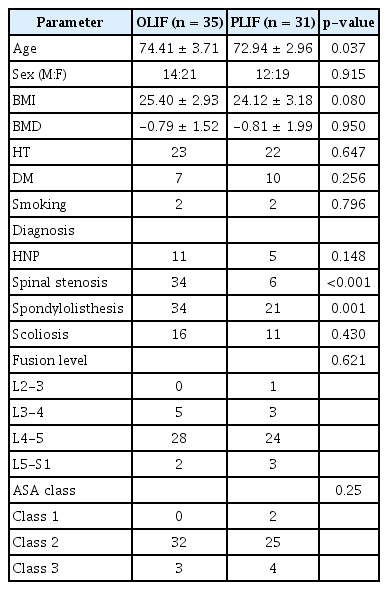
Demographic characteristics
2. Inclusion and Exclusion Criteria
In both patient groups, the inclusion criterion was a symptomatic lumbar degenerative disease with moderate or severe spinal stenosis (grades III and Ⅳ)26). Patients with (1) lower back pain and/or radiating leg pain with neurogenic intermittent claudication; (2) Progressive neurological deficits accompanied by confirmed moderate to severe lumbar stenosis, spondylolisthesis; and (3) Lumbar herniated nucleus pulposus by radiological examinations, were included. Patients with spinal neoplasia, infectious spondylitis, or trauma were excluded.
3. Operative Technique
(1) OLIF
The patient was placed in the right lateral decubitus position and the disc level was checked under fluoroscopy. After a 3 to 4 cm incision in the skin, peritoneal fat was observed inward when the three layers of the abdominal muscles (external oblique, internal oblique, and transverse oblique) were dissected layer by layer. The level of the disc in the surgical field was re-validated and the tubular retractor was located to secure the surgical corridor. First, a discectomy was performed to create sufficient space for the cage. Trials of various sizes were performed to check whether the cage had an appropriate height, width, and angle. The insert cage was then packed with a demineralized bone matrix under fluoroscopy. The abdominal muscles and skin were sutured and the patient was placed in the prone position, and posterior lumbar stabilization was attained via percutaneous pedicle screw fixation14).
(2) PLIF
The procedure was performed in accordance with the conventional method4). Interbody fusion was performed by inserting bilateral cages filled with a demineralized bone matrix and autologous bone blocks. In this study, open pedicle screw fixation was performed to stabilize the posterior lumbar spine.
4. Evaluation of Clinical and Radiologic Outcomes
The clinical outcomes of the two patient groups were analyzed using the hospital's electronic medical records review. Back and leg pain was assessed using a visual analog scale (VAS), and functional impairment due to back pain was assessed using the Oswestry Disability Index (ODI). Additionally, operation time, estimated blood loss (EBL), and length of post-operative hospitalization were investigated. Disc height (DH) was measured as the distance between the middle parts of the lower and upper endplates of the disc, and foraminal height (FH) was obtained by measuring the distance between the upper and lower parts of the inferior and superior pedicle walls in the disc area (Fig. 1)18,29). By comparatively analyzing the pre- and post-operative images, we measured the DH gain (post-operative DH – pre-operative DH), FH gain (post-operative FH – pre-operative FH), DH maintenance (post-operative day [POD] 1-year DH – post-operative DH), and FH maintenance (POD 1-year FH – post-operative FH). Cage subsidence was defined as a DH difference of >2 mm on radiographs immediately post-operative and post-operative 1 year (Fig. 2). In the OLIF group, the cross-sectional area (CSA) was measured using magnetic resonance imaging (MRI) before and one week after surgery, and the results were analyzed (Fig. 3)27).
Disc height (DH): distance between the middle parts of the endplate. Foraminal height (FH): distance between the lower pedicle line of the upper vertebral body and the upper pedicle line of the lower vertebral body.
Cage subsidence. POD: post-operative day.

Cross-sectional area was measured along the thecal sac in T2-weighted magnetic resonance images.
5. Evaluation of Operation-related Complications
Complications were classified into intra-operative complications and post-operative complications. Each complication was prospectively recorded and retrospectively analyzed by referring to well-known complications reported in previously published literature5,19,23).
6. Statistical Analysis
Continuous and categorical variables were expressed as means with standard deviations and frequencies with percentages, respectively. Differences in clinical and radiological outcomes between the two groups were evaluated using Student’s t-test for continuous variables and χ2 and Fisher’s exact tests for categorical variables. In the OLIF group, the change in CSA (mm2) before and after surgery was analyzed using a paired t-test. Statistical significance was set at p value of less than 0.05. All analyses were performed using IBM SPSS Statistics (version 26.0; IBM Corp., Armonk, NY, USA).
RESULTS
1. Clinical Data
Between April 2016 and April 2022, patients aged >70 years underwent OLIF and PLIF at the Yangsan Pusan National University Hospital for degenerative spinal disease. There were 35 OLIFs and 31 PLIFs and the average age of the OLIF group was 74.41±3.71, and that of the PLIF group was 72.94±2.96. The most common fusion levels in OLIF and PLIF were L4–5 (28 and 24 cases, respectively) (Table 1).
The pre-operative VAS and ODI were similar between the two groups. In each group, the VAS and ODI scores tended to improve post-operatively and during the 1-year follow-up. However, there were no significant differences in the VAS and ODI scores between the two groups at 1-year after POD and before surgery. EBL was 162.60±98.20 in the OLIF group, 319.35±197.35 in the PLIF group, and significantly less occurred in the OLIF group. The operation times were similar in the two groups, and the hospitalization period was 14.40±4.24 in the OLIF group and 18.51±8.71 in PLIF group, making that of the OLIF group significantly shorter (Table 2).
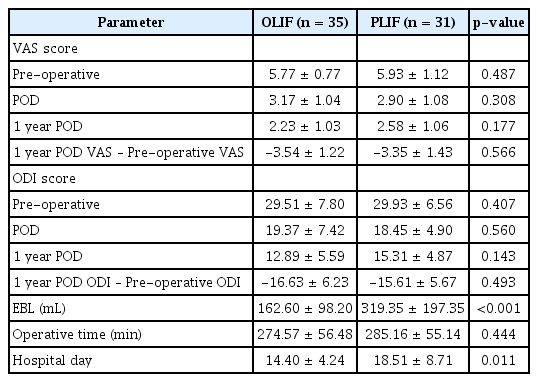
Clinical data
2. Radiologic Data
In the radiologic data, the pre-operative DH and FH were similar. However, DH and FH post-operatively were significantly different between the two groups. DH and FH gains were significantly greater in the OLIF group than in the PLIF group. The DH and FH maintenance was significantly higher in the OLIF group.
In addition, a comparison was conducted by checking whether cage subsidence exceeded 2 mm on POD 1-year radiographs, and there was a significant difference between the two groups (Table 3).

Radiologic parameters
3. CSA
The CSA was compared pre-operative and post-operatively (Table 4). The pre-operative CSA was 57.45±38.66 mm2 and the post-operative CSA was 109.74±40.93 mm2. Accordingly, the CSA has been statistically expanded significantly.

Cross-sectional area changes in OLIF
4. Complications
Psoas paresis and approach-site hematoma occurred predominantly in OLIF. The approach site was the space between the abdominal muscles and the vertebral body. The approach-site hematoma was a subclinical finding, and all four patients with psoas paresis recovered before discharge without treatment. In the PLIF group, dural tears occurred in four patients, two in the operating field and two showed CSF drains into the Hemovac drain. All four patients underwent absolute bed rest and recovered without revision surgery. Details of the complications are divided into intra-operative and post-operative complications and are summarized in Table 5.

Operation-related complications
DISCUSSION
It has been reported that open surgery can produce satisfactory results in elderly patients if proper intra-operative manipulation and active treatment after operation are performed9,28). However, spinal surgery for the elderly can be a complex and delicate procedure that requires careful consideration of various factors, including the patient's age, overall health, medical history, and specific conditions that require surgical intervention25). Bone becomes brittle with age, and the risk of complications associated with surgery increases. In addition, elderly patients may have preexisting medical conditions that could complicate surgery or slow the healing process. From this perspective, open spinal fusion is particularly risky for elderly patients. In elderly patients, it is important to obtain the best results using minimally invasive surgical methods. Minimally invasive spinal surgery has recently been performed on elderly patient1,20,21). Minimally invasive spine surgery is a type of surgical procedure that uses specialized tools and techniques to operate on the spine with minimal damage to surrounding tissues. It is becoming increasingly popular compared with traditional open spinal surgery6,7,15) because it can be used to treat various degenerative spinal diseases, with multiple positive outcomes reported in many papers8,10,17). The advantage of OLIF is that it is performed through a small incision; consequently, there is little tissue damage, relatively little blood loss, and quick recovery time. In addition, indirect decompression can be expected because a larger cage can be inserted than in conventional open spinal fusion30).
We aimed to confirm the usefulness of OLIF in elderly patients. There was no significant difference in the clinical outcomes of the VAS and ODI between the two groups; however, the advantages of OLIF as a minimally invasive surgery were confirmed using various indicators in our study. In elderly patients, EBL and prolonged hospital stay can cause other related complications. In our analysis, the OLIF group had a significantly lower EBL and shorter hospital stay than the PLIF group, although the average age was higher. This point is considered an important aspect when considering the surgical method for elderly patients, because patients can recover relatively quickly, reduce post-operative pain, and improve their quality of life. Several studies have reported that the indirect decompression effect of OLIF can be confirmed by DH, FH, and CSA11,22,27). Radiological evaluation showed that the gain and maintenance of the DH and FH were significantly higher in the OLIF group than in the PLIF group. Because the PLIF group underwent laminectomy before cage insertion, direct decompression was possible; however, this method causes situations that can be risky for elderly patients, such as increased EBL, drainage catheter insertion, and back muscle damage3,13). In contrast, the OLIF group used a larger cage than the PLIF group to increase and maintain the DH and FH, enabling sufficient indirect decompression without laminectomy, which can be considered less burdensome for elderly patients. In addition, the maintenance of DH and FH in the OLIF group and the low incidence of subsidence can be considered to have a low risk of potential pseudoarthrosis since it can lower the possibility of a revision operation; this is considered a meaningful result for elderly patients with a high risk of surgery2,16). MRI was performed at POD 7 to confirm the visible decompression effect. Accordingly, it was possible to measure the change in the CSA pre-operative and on POD 7, and a significant increase was confirmed as a result of the analysis. This supports the idea that OLIF is a minimally invasive procedure with a sufficient decompression effect.
The incidence of intraoperative complications was related to the individual characteristics of the OLIF and PLIF procedures, and as in previous reports, psoas paresis and approach site hematoma occurred in the OLIF group and dural tears in the PLIF group13,14). The incidence and rate of post-operative complications were low in the OLIF group. Post-operative complications in elderly patients can affect prognosis, and low post-operative complications suggest that OLIF is a relatively safe surgical method for elderly patients.
Our study has several limitations. First, because the study was conducted at a single center, the sample size was insufficient, multilevel fusion was not included, and a retrospective study was conducted with a relatively short follow-up period. Second, although OLIF and PLIF represent open spine surgery and minimally invasive surgery, respectively, bias may occur because they do not represent all surgeries. Third, in addition to DH and FH, other radiological outcome factors, such as sagittal balance and lordosis, were not analyzed. Fourth, the types of complications that occurred in the OLIF and PLIF groups were identified; however, the severities of the complications were not compared.
Each surgeon preferred a specific surgical method. Additionally, the decision to perform spinal surgery in the elderly should be made on a case-by-case basis, with careful consideration of the risks and benefits involved. However, since there are few domestic comparative studies between conventional and minimally invasive spinal fusion in elderly patients over 70, this study is considered a reference when deciding on spinal fusion in elderly patients.
CONCLUSION
The elderly population is increasing worldwide and Korea has become a super-aging society. Reflecting on this aging society, the need for spinal interbody fusion has increased, especially among elderly patients, with many surgeries are being performed. Accordingly, the burden on surgeons in the operation of elderly patients is significant. Although the clinical results in this study did not differ from those of conventional open spinal fusion surgery, OLIF enabled sufficient indirect decompression, less EBL, shorter hospitalization, and less subsidence. OLIF is thought to be a beneficial, minimally invasive surgical method for elderly patients who need spinal fusion but are reluctant to undergo surgery because of this risk.
Notes
No potential conflict of interest relevant to this article was reported.