Incidence and Predictors of Kummell’s Disease in Patients with Benign Vertebral Compression Fractures
Article information
Abstract
Objective
Kummell's disease (KD) is a form of delayed vertebral compression fracture. However, its incidence and predictors remain unclear. We investigated the incidence rate and predictors of KD in patients with benign vertebral compression fractures.
Methods
We retrospectively analyzed 437 consecutive patients with benign vertebral compression fractures admitted to the neurosurgical department of Nowon Eulji Medical Center between 2015 and 2018. The inclusion criterion was patients with newly diagnosed KD at ≥20 years of age. The control subjects had acute benign vertebral compression fractures. Univariate and multivariate regression analyses were performed to evaluate the predictors of KD.
Results
In total, 39 patients (8.9%) were newly diagnosed with KD, with an average age of 77.3 years. In older patients (≥70 years), the incidence was 12.8%. The incidence rate was highest in patients in their 70s. Most cases of KD (69.2%) occurred in the thoracolumbar region. Multivariate regression analysis showed that age ≥70 years (odds ratio [OR], 3.24; 95% confidence interval [CI], 1.05–9.97; p=0.041) and a history of ischemic stroke (OR, 2.92; 95% CI, 1.26–6.74; p=0.012) were independently associated with KD.
Conclusion
KD appears to be relatively common, especially in older people (≥70 years). Older age and a history of ischemic stroke may be independent predictors of KD. This study also indicated that ischemic factors may play a more important role than mechanical factors in the development of KD from vertebral compression fractures.
INTRODUCTION
Kummell's disease (KD), described first in 1891 by German surgeon Hermann Kummell, was well known as 'delayed post-traumatic vertebral osteonecrosis' after vertebral compression fracture, resulting in a painful, progressive kyphotic deformity that lasted for a few weeks or months28). KD is a type of delayed vertebral compression fracture characterized by late-onset vertebral body collapse10,27). The progression of KD from vertebral compression fracture can be divided into the following stages13,28,34): After a vertebral compression fracture occurs, usually due to an injury, there may be a period of symptom relief, and the patient may be asymptomatic. Consequently, the affected vertebral body may collapse, leading to kyphotic deformity. As the disease progresses, the patients may experience long-term back pain and neurological deficits.
KD is a reportedly rare disease according to previous literature26). However, as the aging population increases, the incidence of KD may become much higher than previously reported. Recently, it has been reported that it ranges widely from 7% to 37% of vertebral compression fractures7,17,22,23,32), but the incidence of KD from vertebral compression fractures is still unclear.
KD is caused by primary mechanical factors and subsequent ischemic events that lead to necrosis of the vertebral body19,25). It has been associated with osteoporosis5,6,23,29), steroid therapy19,23,26), vasculitis or hemoglobinpathy2,5,23), radiation therapy4), chronic alcoholism4,19,23), pancreatitis4), liver cirrhosis4), diabetes mellitus4,35), malignancy4), infection4), and sarcoidosis12). However, to date, contributing factors to KD from vertebral compression fractures remain unclear.
This study aimed to investigate the incidence and predictors of KD in patients with benign vertebral compression fractures.
MATERIALS AND METHODS
1. Study Population
We retrospectively analyzed 437 patients with benign vertebral compression fractures admitted to the neurosurgical department of Nowon Eulji Medical Center between January 2015 and December 2018. Of these, 39 were newly diagnosed with KD. The inclusion criteria were: 1) patients with newly diagnosed KD; and 2) ≥20 years. The exclusion criteria were the presence of infections and malignancies. KD and acute benign vertebral compression fractures were diagnosed using simple radiography, computed tomography (CT), or magnetic resonance imaging (MRI) by neurosurgeons and confirmed by a diagnostic radiology specialist. The control subjects (n=405) were admitted with acute benign vertebral compression fractures during the same period.
2. Definition
'KD' was defined as the presence of an intravertebral cleft on simple lateral radiography or CT or the evidence of osteonecrosis with a fluid sign in the vertebral body on MRI or a diffuse low-signal intensity on T1-weighted MRI1,24,32,34).
3. Data Collection
We collected demographic, clinical, and laboratory data from the electronic medical record system, radiological data from simple radiography, CT, or MRI, and bone mineral density (BMD) data from a Picture Archiving and Communication System. 1) age; 2) sex; 3) height; 4) weight; 5) trauma history; 6) onset of injury; 7) medical history including hypertension, diabetes mellitus, hyperlipidemia, history of coronary artery disease or ischemic stroke; 8) admission period; 9) vertebroplasty or kyphoplasty; 10) hemoglobin level; 11) platelet count level; 12) C-reactive protein level; 13) acute vertebral compression fracture; 14) presence of previous vertebral fracture; 15) level of fracture; 16) level of KD; and 17) T-score of the spine or femur neck.
4. Statistical Analysis
We used the χ2 test for nominal variables, the independent t-test for continuous variables, and the Mann-Whitney U test for nonparametric variables. Univariate regression analysis was performed for old age ≥70 years, hypertension, coronary artery disease, ischemic stroke, presence of previous vertebral fracture, and osteoporosis T-score ≤-2.5. To assess independent predictors of KD from vertebral compression fractures, multivariate regression analysis was performed after adjustment for age ≥70, ischemic stroke, presence of previous vertebral fracture and osteoporosis, T-score ≤-2.5. Hypertension and coronary artery disease were not included as covariates because of their high possibility of multicollinearity with ischemic stroke. Odds ratios (OR) and 95% confidence intervals (CI) were determined. A p-value of less than or equal to 0.05 was considered statistically significant. Statistical analyses were performed using SPSS (version 27.0; IBM Corp., Armonk, NY, USA).
5. Ethics Statement
This study was approved by the Institutional Review Board (IRB) of the Nowon Eulji Medical Center (IRB No. 2023-11-010-001).
RESULTS
1. Incidence of KD
A total of 437 patients with benign vertebral compression fractures were analyzed. Of these, 39 patients (8.9%) were newly diagnosed with KD. In the older population >70 years, the crude incidence rate of KD increased to 12.8%. Its incidence rate peaked in the 70s category (14.4%), with an average age was 77.3 years. Fig. 1 shows the age-specific incidences of KD. This disease occurred three times more frequently in females than males (76.9% vs. 23.1%, respectively). Most cases of KD (69.2%) occurred in the thoracolumbar region. Table 1 shows the baseline data of 437 patients with vertebral compression fractures.
Age-specific incidence of Kummell's disease.
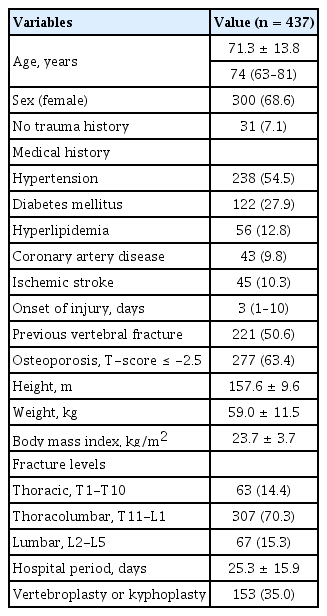
Baseline data of 437 patients with vertebral compression fractures
2. Univariate Analysis
Age, ischemic stroke, and to a lesser extent, hypertension, history of coronary artery disease, presence of previous vertebral fracture, and osteoporosis, T-score ≤-2.5 significantly differed between KD and acute simple vertebral compression fracture. Table 2 shows the clinical and radiological characteristics of 39 patients with KD.
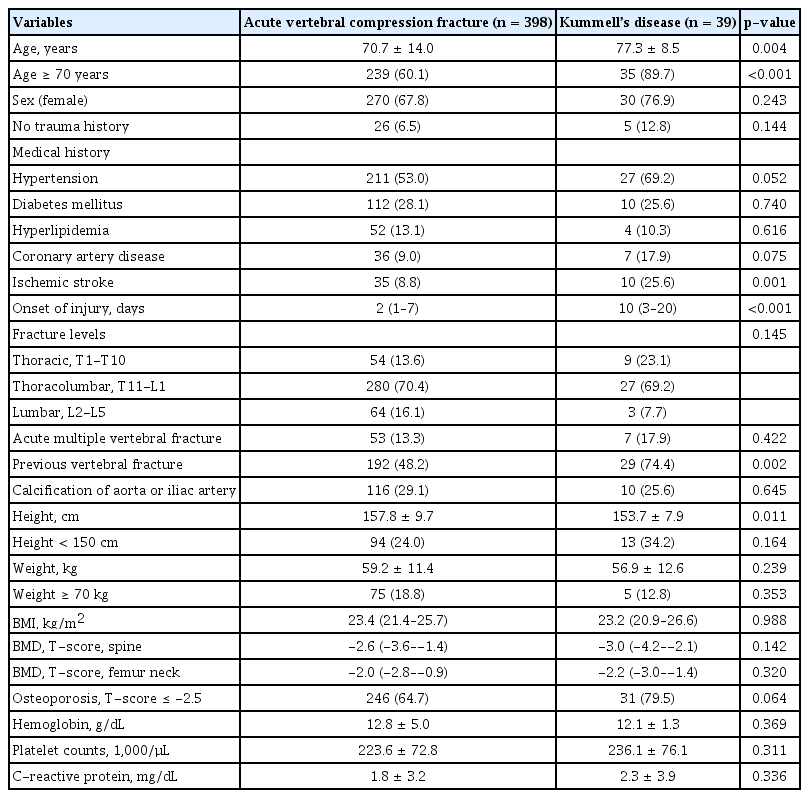
Clinical and radiological characteristics of 39 patients with Kummell’s disease
Univariate regression analysis showed that old age ≥70 years (OR, 5.82; 95% CI, 2.03–16.70; p=0.001), hypertension (OR, 1.99; 95% CI, 0.98–4.05; p=0.056), history of coronary artery disease (OR, 2.22; 95% CI, 0.91–5.34; p=0.081), history of ischemic stroke (OR, 3.58; 95% CI, 1.61–7.94; p=0.002), presence of previous vertebral fracture (OR, 3.11; 95% CI, 1.48–6.56; p=0.003), osteoporosis, T-score ≤-2.5 (OR, 2.11; 95% CI, 0.94−4.72; p=0.069) were associated with KD.
3. Multivariate Analysis
In multivariate regression analysis, old age ≥70 years (OR, 3.24; 95% CI, 1.05–9.97; p=0.041) and history of ischemic stroke (OR, 2.92; 95% CI, 1.26–6.74; p=0.012) and to a lesser extent, presence of previous vertebral fracture (OR, 2.02; 95% CI, 0.92–4.44; p=0.082) were independently associated with KD. Table 3 shows multivariate regression analysis for KD.
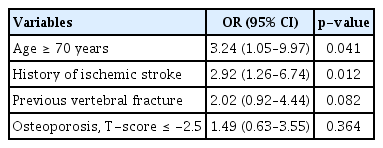
Multivariate regression analysis for Kummell’s disease
DISCUSSION
Our findings reveal that KD may be relatively common, particularly in older people above 70 years. Old age ≥70 years and a history of ischemic stroke may be independent predictors of the development of KD from benign vertebral compression fractures. Currently, there are several studies on the incidence of KD and its pathogenesis from benign vertebral compression fractures7,17,22,23,32). However, there are few studies on the predictors of the development of KD from benign vertebral compression fractures. In our findings, we believe ischemic stroke has a strong association with KD from benign vertebral compression fractures.
1. Incidence of KD
Although the incidence of KD is known to be uncommon, recently, it has ranged widely from 7% to 37% of vertebral compression fractures in elderly people1,7,17,22,23,32). Some studies reported that nonunion from osteoporotic vertebral compression fractures ranges from 13.5% to 19.6%14,31). In a retrospective study of 652 consecutive patients with osteoporotic compression fractures, 67 (10.3%) had an intravertebral vacuum phenomenon that occurred predominantly in the thoracolumbar region17). In our study, the incidence of KD was 8.9% in adult patients and increased to 12.8% among older adults ≥70 years. The actual incidence in the older population may be much higher than previously reported due to the rapid increase in the number of older people. KD usually affects the thoracolumbar junction of the spine. Our findings show the majority of KD (69.2%) occurred in the thoracolumbar junction. It seems to be due to physiologic kyphosis or the inherent vulnerability of ischemia of the thoracolumbar region.
2. Aging
The aging process may be associated with the development of KD. Bone aging is usually caused by decreased blood supply to the bone18) and loss of progenitor cells of the bone6,23). Aging leads to various structural changes in blood vessels, such as atherosclerosis, stiffness, luminal narrowing, and deterioration of the structural integrity of the blood wall2,23). Additionally, a decrease in bone mass due to aging may reflect a decrease in osteoblasts due to the loss of progenitor cells in the bone6,23). This aging process may lead to the failure of the repair mechanism of the fractured vertebral body, culminating in the development of KD. This study suggests that old age ≥70 years may be a strong independent predictor of KD in patients with vertebral compression fractures.
3. Ischemic Factors
KD is an ischemic disease of the vertebral body. A robust blood supply is essential for vertebra to maintain their anatomical structure and function2,23). There is no doubt that ischemic stroke is an advanced-stage vascular disease. Therefore, atherosclerosis as a systemic disease may be associated with ischemic bone disease. Additionally, vertebral compression fractures can cause fatty microembolisms that occlude blood vessels within the vertebra, worsening the blood supply to the vertebra21,23,26). This negatively impacts the healing of the fractured vertebral bone and increases the possibility of progression to KD26). KD has been reported to be associated with rare vasculitis or hemoglobinpathy2,5,23). On the other hand, our findings suggest a strong association between ischemic stroke and KD in patients with vertebral compression fractures. It is thought that ischemic stroke may have the effect of lowering the blood supply to the bone as a systemic disease, including atherosclerosis, stenosis, or occlusion of the blood vessels in the whole body23,26,34).
The differences between coronary artery disease and ischemic stroke are diverse in terms of its causes and pathogenesis. The possible causes of ischemic stroke are more heterogeneous than those of coronary artery disease. Coronary artery disease is almost always the result of unstable plaque in the affected arteries. Hyperlipidemia is a well-documented risk factor for coronary artery disease than in ischemic stroke20). In contrast with coronary artery disease, the principal mechanisms for ischemic stroke are large artery atherosclerosis, cardiac embolism, and small vessel diseases33). Less commonly, ischemic strokes may be also caused by vasculitis, arterial dissection, and hypercoagulability. In small vessel disease of the brain, the main etiology is the existence of microatheroma in the penetrating arteries of the deep brain structures8). Similarly, the microatheroma formation in the small feeding artery of the vertebral bone may be non-union or focal osteonecrosis of the fractured vertebral bone.
4. Osteoporosis
Osteoporosis has been strongly associated with KD5,6,23,28). In patients with osteoporosis, healing after a compression fracture is commonly delayed due to insufficient levels or diminished activity of osteoblasts, which are essential for bone healing, and an intravertebral vacuum cleft may appear more frequently as the bone density reduces6,23). Weakened vertebrae with osteoporosis are considered contributing factors to KD in older adults22,23,26). In our study, osteoporosis was higher in KD than in control group (79.5% vs. 64.7%, p=0.064) and was associated with KD (OR, 2.11; 95% CI, 0.94−4.72; p=0.069), but was not an independent predictor in multivariate regression analysis. This may be due to the small number of cases of KD or frequent false-negative findings of BMD measured using dual energy X-ray absorptiometry, which is caused by osteophytes or calcification of the lumbar spine or the aorta. Gou et al.9) reported that a teriparatide injection of 12 months significantly decreased back pain and the size of intravertebral clefts in 21 patients with KD. Therefore, it is recommended that anabolic agents such as teriparatide or romososumab should be administered in patients with KD.
5. Mechanical Factors
A history of previous vertebral fractures substantially increases subsequent fracture risk beyond that explained by BMD11,15,16). A biomechanical study reported that kyphotic deformity caused by a prior vertebral compression fracture may result in subsequent fractures in the vertebra below the fracture site due to increased compression force3). In our study, the prevalence of previous vertebral fractures was higher in patients with KD, but its association with KD was unclear.
A high body mass index can contribute to increased physical stress on the spine, primarily due to excess weight7,30). Although this condition is often associated with degenerative disc disease, it can also contribute to the progression of vertebral collapse in KD7,30). Some studies have reported that osteonecrosis can occur regardless of compression fracture and that the mechanical characteristics of the thoracolumbar region, rather than vascular occlusion, cause instability within the vertebral body, leading to KD2,23,27). However, in our study, ischemic factors such as ischemic stroke were independently associated with KD, while the various mechanical factors, including the thoracolumbar region, previous vertebral fracture, height, weight, or body mass index, were not related to KD. Our findings indicated that ischemic factors play a more important role than mechanical factors in the development of KD from vertebral compression fractures.
This study had several limitations. First, this was a retrospective, single-center study with a small sample size; therefore, selection bias may have occurred. Large multicenter studies are required to validate predictors of KD. Second, chronic use of steroids can cause fat accumulation in the vertebral body, impair blood flow in the bone marrow21,26), and lead to atherosclerosis in the medullary arterioles where fat is accumulated23,26). However, in our study, the impact of steroids on KD could not be investigated because of the lack of such cases. Radiation, alcoholism, pancreatitis, and liver cirrhosis were not evaluated for the same reason.
CONCLUSION
In our study, KD was relatively common, especially in older individuals. Old age (≥70 years) and a history of ischemic stroke, may be independent predictors of the development of KD from benign vertebral compression fractures. Our findings indicate that ischemic factors rather than mechanical factors play a more important role in the pathogenesis of KD from benign vertebral compression fractures. Further multicenter studies are required to support our findings and consider other confounding variables.
Notes
No potential conflict of interest relevant to this article was reported.