INTRODUCTION
Diffuse idiopathic skeletal hyperostosis (DISH) is a common skeletal disorder in the elderly population and is characterized by flowing anterolateral ossifications alongside the right thoracic spine, frequently accompanied by similar ossifications of the remaining spinal segments and peripheral tendinous insertion4,8,10,12,13). Although generally asymptomatic, large cervical anterior osteophytes have been reported to cause swallowing disorders11,14). Surgical resection of the osteophytes was reported to be an effective treatment. However, postsurgical recurrence of cervical osteophytes causing dysphagia with long-term follow-up has also been reported11). A regrowth rate of 1mm/year after surgical resection of osteophytes in 20 segments of 7 patients with DISH was reported.
Heterotopic ossification (HO) refers to bone formation in tissues that normally do not exhibit osteogenesis15). HO is a well-known complication of total hip arthroplasty (THA) and its incidence varies greatly from 2% to 53% following THA5,15). It has also attracted clinical attention since the introduction of total disc replacement (TDR), which was designed to preserve segmental motion and theoretically prevent adjacent segment degeneration of the cervical spine following surgery for cervical spondylosis and disc disease5,15). However, the incidence and clinical implications of HO following anterior cervical fusion (ACF) in patients with DISH has not been investigated. We report a case of extensive HO following ACF in a patient with DISH.
CASE REPORT
A 59-year-old male patient presented with chronic refractory pain associated with bilateral arm and leg following cervical spinal cord injury. He had sustained a motor vehicle accident five years ago and became quadriplegic due to cervical cord contusion at C4 level (upper extremities, NMT grade II/lower extremities, grade 1). He underwent decompression and ACF from C3 to C6 five days after the accident. His neurologic condition did not improve postoperatively. He was rehabilitated in several hospitals, subsequently. Persistent and chronic neuropathic pain triggered by spinal cord injury developed within a month after cervical spinal trauma. The pain was described as mainly stabbing and cold with a severity of 8 to 9 out of 10 on a numerical rating scale ranging from 0 to 10. It was not aggravated with neck motion. Spontaneous cold pain was detected in his bilateral hand and fingers, upper thoracic area, and bilateral legs. Mechanical and cold allodynia was present in his bilateral palms and fingers, consistent with at-level neuropathic pain. Chronic at-level and below-level neuropathic pain was not relieved with maximal medical treatment including gabapentin (1,800mg/day), pregabalin (450 mg/day), tramadol (300mg/day), amitriptyline (20mg/day), and OxyContin (40mg/day) and transdermal fentanyl (50mcg/day). He was referred to our department for pain control.
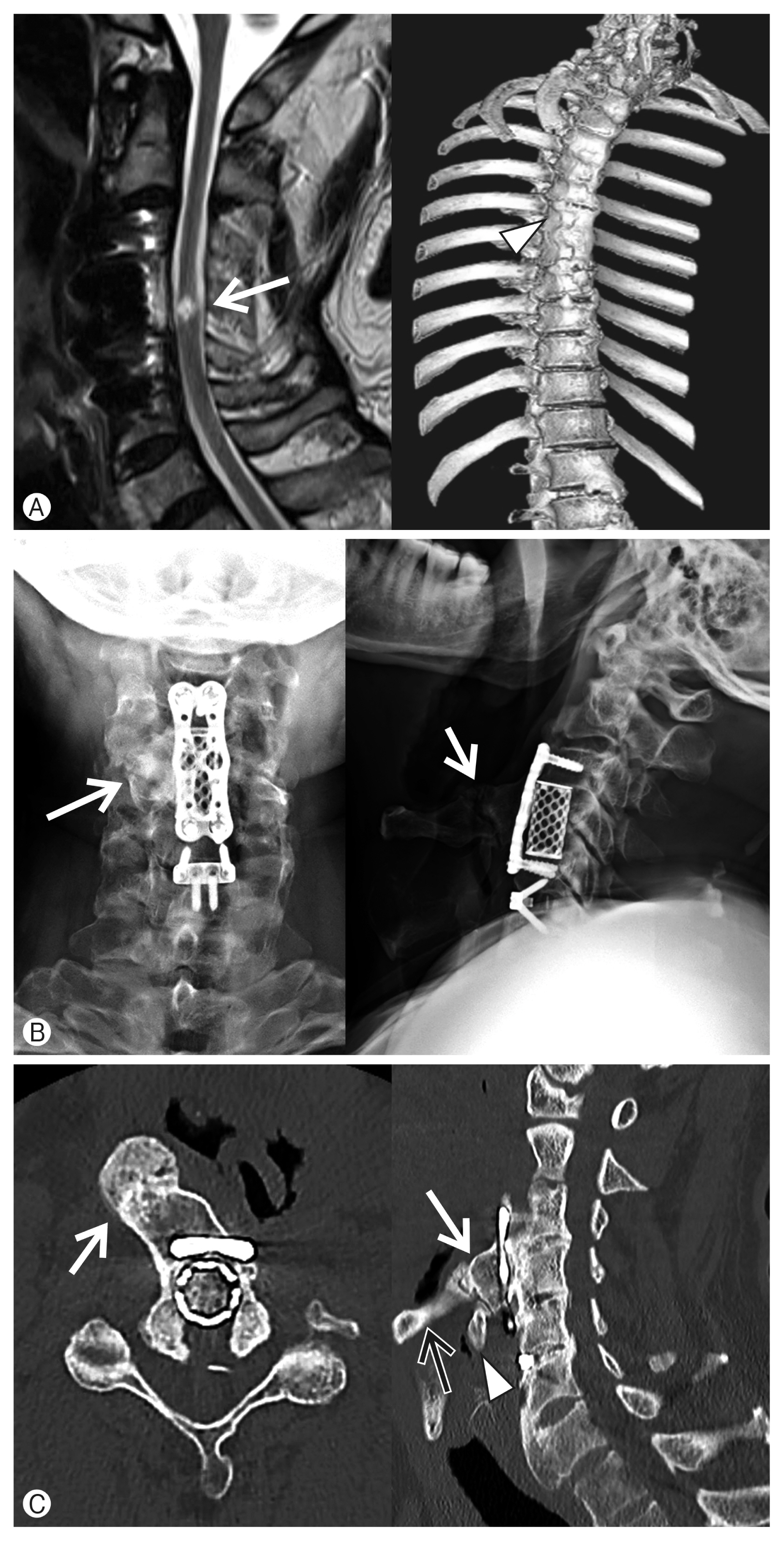
He showed typical features of complete spinal cord injury at C4/5 at the time of presentation (64 months postinjury). He could not manage his routine daily activities, including eating, washing, and moving. Caregiver assistance was needed in most of his activities of daily living. His medical history was unremarkable, including diabetes, gout, and so on. During examination, he complained of chronic swallowing difficulty since the accident and the operation. Indeed, despite of several years of rehabilitation treatment, his swallowing difficulty was not improved. He has had difficulty in swallowing solid food after the accident and ACF. No evidence of airway obstruction was evident. His cervical x-ray examination at the time of presentation showed a prominent anterior cervical osteophyte at the level of C4/5 (Fig. 1). Computed tomographic (CT) scan of the neck showed a large anterior cervical osteophyte growing from the C4 corpectomy site to the right hyoid bone. Due to large osteophyte, the wall of posterior pharyngeal space was displaced medially. Pseudoarthrosis was found between the osteophyte and hyoid bone. Retrospective evaluation of DISH and HO was performed. The CT scan of the thoracic spine showed a longitudinal osteophyte along the right anterolateral vertebral column, consistent with DISH (Fig. 1)
Preoperative cervical spine x-ray and CT scan showed the presence of large osteophyte from C4 to C7, which was consistent with DISH, and ossified posterior longitudinal ligament (OPLL) along C4 to C6 with resultant cervical spinal stenosis (Fig. 2). Resection of large anterior cervical osteophyte from DISH and decompression of cervical spinal cord with removal of OPLL was performed by C4 corpectomy with C4 to C6 interbody fusion with mesh cage and an additional anterior cervical discectomy and fusion at C6/7. The large anterior osteophyte was successfully via cervical anterior decompression and fusion (Fig. 2). However, in the cervical x-ray obtained one year after the ACF, regrowth of the anterior cervical osteophyte was evident at the C4 level (Fig. 2). A follow-up lateral x-ray of the cervical spine 32 months after the ACF revealed more extensive anterior growth of osteophyte abutting the hyoid bone, revealing a pseudoarthrosis (Fig. 2). Regrowth of the anterior osteophyte from DISH appears to have started after the ACF and with progressive enlargement.
Due to progressive growth of the osteophyte and presence of continued swallowing difficulty over 5 years after ACF, surgical resection was considered. However, the patient refused to undergo surgery of the cervical spine and regular follow-up was planned. The chronic neuropathic pain responded positively (>50% pain relief) with intrathecal infusion of morphine sulfate. After repeated trial of intrathecal infusion of morphine and confirmation of treatment efficacy, permanent implantation of intrathecal drug delivery system was performed. The patient reported about 30% to 40% pain relief at 6 months post-implantation despite maximal medical treatment. His swallowing difficulty did not show any change and annual follow-up was planned.
DISCUSSION
1. DISH and Anterior Cervical Osteophytes
DISH is a poorly understood, systemic condition characterized by progressive calcification and ossification of ligaments and enthuses8). The formal diagnosis of DISH is established radiologically based on simple descriptive morphological abnormalities of the thoracic spine12,13). Although DISH is a largely asymptomatic condition, increasing evidences suggests that DISH was an indicator of several pathological conditions8). The presence of DISH may indicate underlying metabolic derangement and cardiovascular disease. Moreover, bone deposition may lead to biomechanical changes of the musculoskeletal system and the formation of obstructive cervical masses8,17). Several risk factors, including male sex, hypertrophic osteoarthritis, and ankylosing spondylitis have been suggested in the literatures.
The mechanism of swallowing difficulty due to large cervical osteophytes is still unknown. However, a variety of mechanisms have been suggested, including direct mechanical compression of the pharynx and esophagus12), disturbances of normal epiglottis tilt over the laryngeal inlet by the osteophytes at C3 and C4 level6,14), tissue inflammation around the esophagus1), and cricopharyngeal spasm1). The incidence of dysphagia in patients with DISH ranged between 17% and 28%9,12). Conservative treatment is indicated for the initial management. Surgical decompression via osteophytectomy is an effective treatment for patients with severe dysphagia and airway obstruction1,3,6,9,11,16,18).
Although simple surgical resection of the osteophytes has been effective in relieving dysphagia, long-term recurrence of osteophytes with dysphagia after 10 years following osteophytectomy has also been reported11). After a mean follow-up period of 9 years (range, 6-13 years) in seven patients with severe dysphagia, who underwent surgical resection of the cervical anterior osteophytes accompanying DISH, radiological recurrence of osteophytes occurred, with an average increase rate of approximately 1mm/year following resection11). Two out of seven patients developed recurrent dysphagia along with osteophyte formation11). The incidence of recurrent osteophytes was significantly higher in the 16 segments with preserved mobility than in four segments without mobility11). Because the incidence of recurrent osteophyte is lower in fused intervertebral segments11), studies suggested that osteophytectomy and fusion was effective in relieving dysphagia and recurrence after resection in patients with DISH. However, it is still inconclusive because of small sample size (6 patients) and short follow-up was short (23±8 months).
2. HO
HO refers to the bone formation outside the skeletal system. In the cervical spine, following fusion or artificial disc replacement, it may consist of ectopic bone formation anywhere around the implant15). The incidence of HO following cervical TDR was reported as high as 66% of patients to none15). Tu et al.15) reported about 50% incidence of HO with more than 96% of these levels remaining mobile with no adverse effect on the clinical outcome. Multi-level surgery, male sex, old age, trauma to the longus colli muscle, hypertrophic osteoarthritis, ankylosing spondylitis, extensive bone removal, and DISH have been implicated in the development of HO15).
Reflecting systemic bone-formation, patients with DISH have a greater propensity to develop HO in response to local events, including joint replacement surgery2,8). Occurrence of HO in joint replacement surgery impairs the function of the affected joint and prophylactic treatment with irradiation or non-steroidal anti-inflammatory drugs may be indicated for such patients2,7,8). It is currently unknown what causes the formation of HO. However, it was suggested that surgical trauma may induce ossification via unknown mechanisms7). To prevent HO, ample irrigation and implantation of anterior cervical plate at least 5mm away from the adjacent disc space have been suggested for patients with DISH who underwent ACF5).