INTRODUCTION
Caudal epidural injection (CEI) is commonly used to manage patients with low back and leg pain and is simple and safe, and has broad indications1). Nevertheless, complications varying from minor to major, such as hypotension, bradycardia, transient headache, epidural or subdural hematoma, cauda equine syndrome (CES), or paraplegia, can develop after the procedure3). Some authors have reported subdural hematoma occurred after the procedure5,8,9). However, to the best of our knowledge, few case reports have been released on subdural-extra arachnoid hematoma after CEI. Here, we describe our experience of the surgical treatment of subdural-extra arachnoid hematoma occurring after CEI.
CASE REPORT
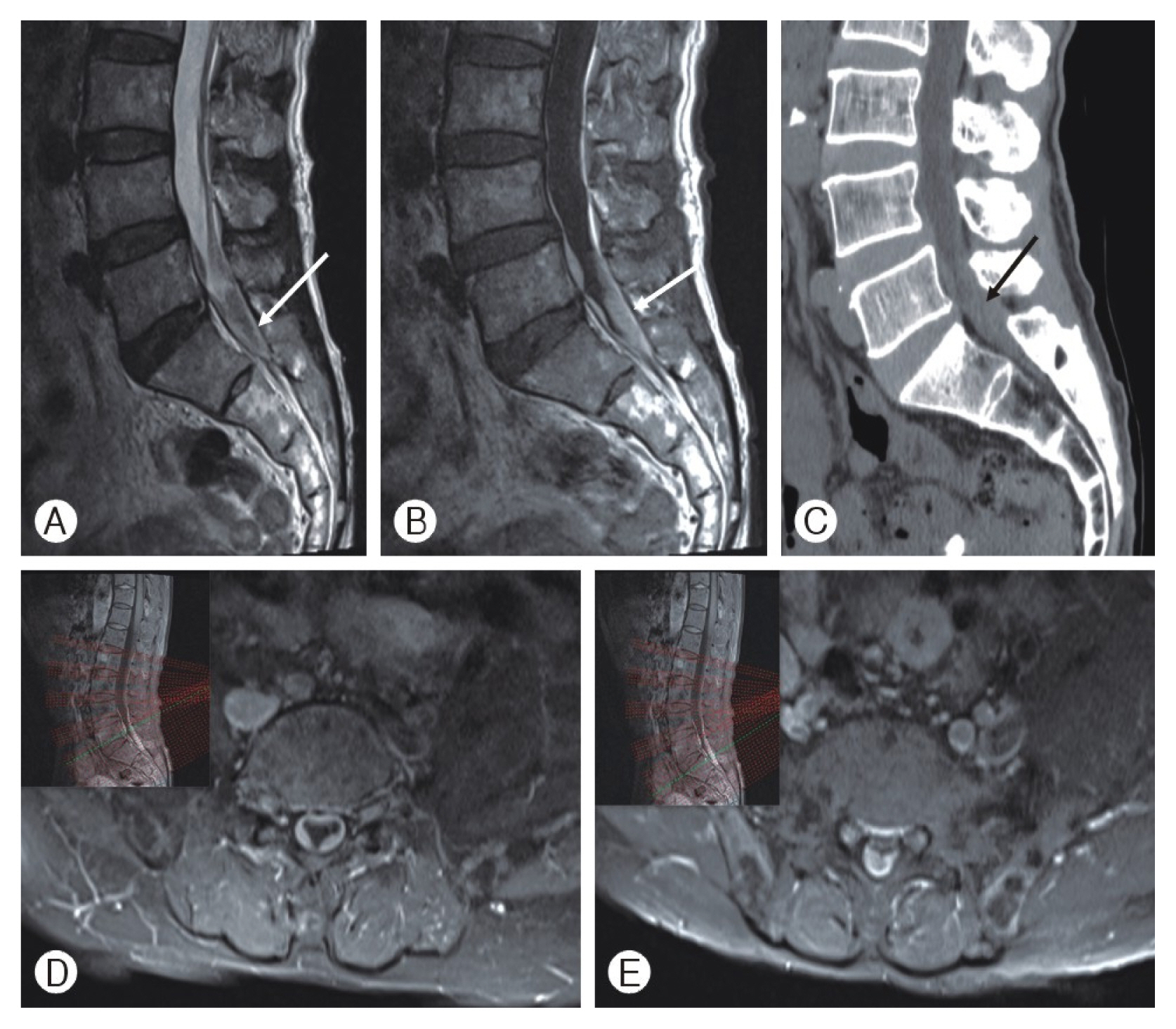
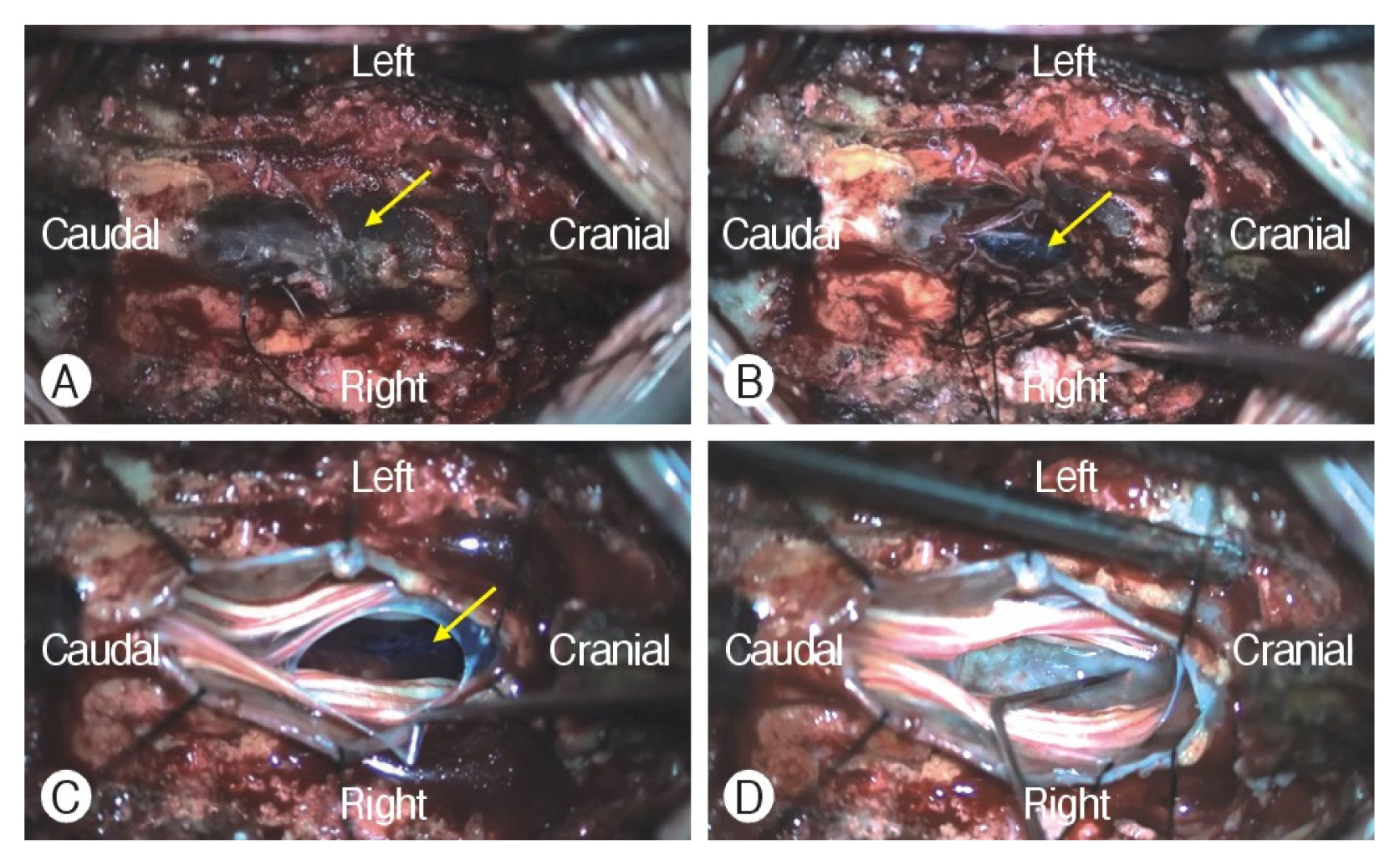
A 71-year-old man complaining of voiding difficulties and radiating pain in both legs visited our outpatient department. He had undergone cardiac stent insertion 8 years previously and had been taken clopidogrel afterward. He had received CEI for low back and right lateral calf radiating pain at another hospital nine days ago. However, low back and right leg pain was aggravated, left leg pain was newly developing after CEI. The next day the patient recognized voiding and defecation difficulties, and felt pain and numbness of saddle area such as CES. The patient waited for days expecting to get better as taking the medicine, but it did not improve. When he revisited the hospital, the doctor recommended our hospital for further evaluation. In neurologic examination, weakness of both legs was absent, but pain and numbness of both posterior thigh and saddle area. Deep tendon reflex was within normal limit. Anal tone was decreased slightly in rectal exam. Lumbar magnetic resonance imaging (MRI) showed subdural hematoma at the L5-S1-S2 level, and computed tomography depicted high density at the same level (Fig. 1). A red pin point was found at coccygeal area as predicting the insertion point of caudal block. The patient underwent emergent surgical treatment for hematoma evacuation at L5-S1-S2 level. A dark brown thecal sac was found after L5 left hemilaminectomy and S1 total laminectomy, and S2 bilateral partial laminectomy (Fig. 2A). Dural incision was performed meticulously, and subdural hematoma was removed, but the arachnoid membrane was intact and clear cerebrospinal fluid (CSF) was observed (Fig. 2B). After CSF gushed out, the dark brown hemorrhage was observed at the bottom of surgical field (Fig. 2C). We found that hematoma occupied the region between the subdural and extra arachnoid spaces. The arachnoid membrane at the bottom side was dissected using a blunt hook, and subdural hematoma completely removed (Fig. 2D). Dura was meticulously sutured using the water-tight method and the suture-site was reinforced using fat tissue and fibrin glue. The surgery was completed without any complications. At postoperative day (POD) one, both leg radiating pain disappeared and the numbness of saddle area was subsided. The patient was absolute bed rest for 6 days because CSF leakage was observed at drain bag. After bed rest, the foley catheter was removed, and the patient started to ambulate. The voiding and defecation difficulty improved incrementally at POD8, and finally voiding and defecation difficulties, and leg pain had completely resolved without any medication at POD14.
DISCUSSION
Spinal subdural hematoma is a rare complication after CEI, and sometimes it manifests as a discordant lesion from the site of injection5). Several factors such as anticoagulation, a wet-tap violating the thecal sac, high-pressure injection into sacral hiatus, or vascular anomalies, are known to contribute to the risk of subdural hematoma4).
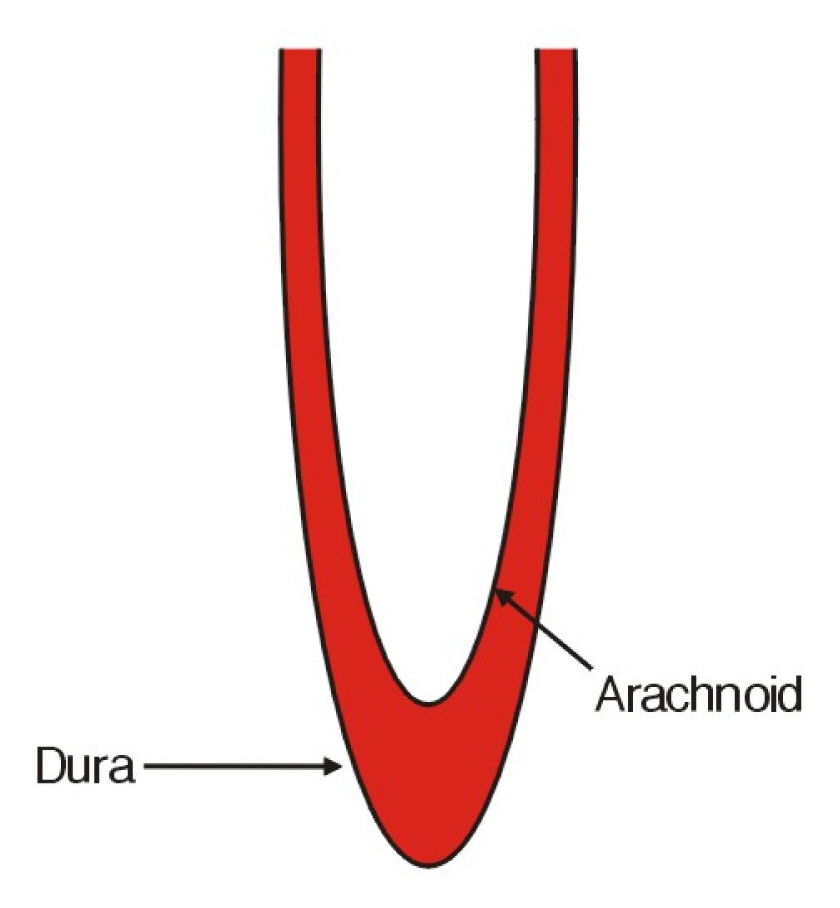
In our case, a dark brown thecal sac was observed in the surgical field, but CSF was transparent and the arachnoid membrane was intact. We intraoperatively found out subdural-extra arachnoid hematoma, which was not revealed on lumbar MRI (Fig. 3). We believe that a wet-tap occurred during the procedure and the needle tip violated the interspace between dura and arachnoid, and caused subdural-extra arachnoid hematoma. Moreover, the anticoagulant (clopidogrel) probably facilitated bleeding at the wet-tap site. Spinal subdural hematoma may occur in several ways, though we believe the above explanation is most plausible in our case. Therefore, we recommend the needle tip does not exceed the upper plate of the Sacral third segment to prevent wet-tap and that iodine epidurography should also be performed before CEI.
In our experience, it is difficult to recover CES that have lasted for more than one week. Nevertheless, symptoms resolved well in our patient. In our opinion, the clinical outcomes of subdural hematoma depend on whether the hematoma occurs within or outside the arachnoid membrane. Subdural and subarachnoid hematoma usually has poor clinical outcomes resulting from severe edema and swelling of nerve rootlets. Moreover, there are the high possibility that the remnants of the hematoma cause an inflammatory response and adhesion of rootles later. However, these findings was not obser ved during surgery in our case, which probably explains the betterthan-expected clinical outcome achieved. Accordingly, clinical outcomes of spinal subdural hematoma would vary depending on the violation of arachnoid membrane.
There were several case reports that stated similar complication after CEI. Occurring CES after CEI can be caused by various pathologies. We summarized case reports in Table 1. Lee et al.6) reported that existing herniated intervertebral disc and injected fluid could cause CES after CEI. Bilir and Gulec2) stated that space-occupied lesion formed by injected fluid would make transient neurologic deficit. Seo et al.7) also reported that neurotoxicity came from local anesthetics could induce CES. The patient was left with a permanent neurological deficit despite of emergent surgical treatment. Chen et al.4) stated that subdural hematoma resulting from tearing fragile vessel by high pressure-injection could cause CES. Finally, we added our case that subdural-extra arachnoid hematoma might be formed after CEI could be one reason of CES. Furthermore, clinical outcome may especially be good in this case.