INTRODUCTION
Turner syndrome is characterized by the absence of the X chromosome in all cells (45,XO genotype). These patients present with short stature, truncal obesity, gonadal dysgenesis, premature ovarian failure, and micrognathia. Half of these patients have aberrant vascular comorbidities, commonly involving the cardiovascular system3,5,7,9,10,13). However, vascular abnormalities of the neurovascular system presenting as potentially life-threatening complications are rare. Here, we present a rare case of subarachnoid hemorrhage (SAH) as a manifestation of cerebral aneurysm rupture in a patient with previously diagnosed Turner syndrome.
CASE REPORTS
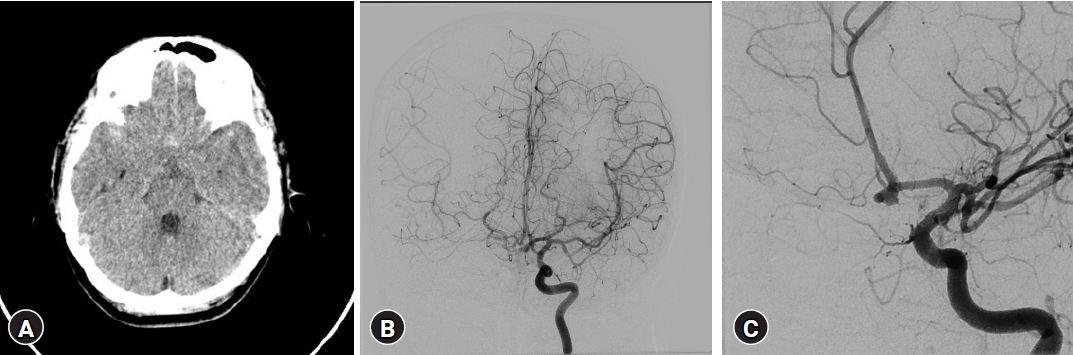
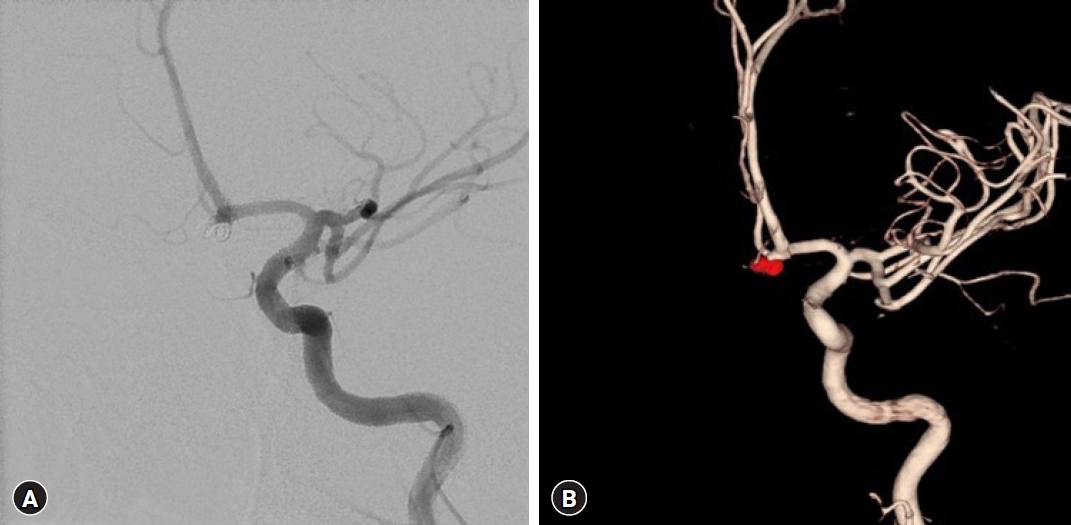
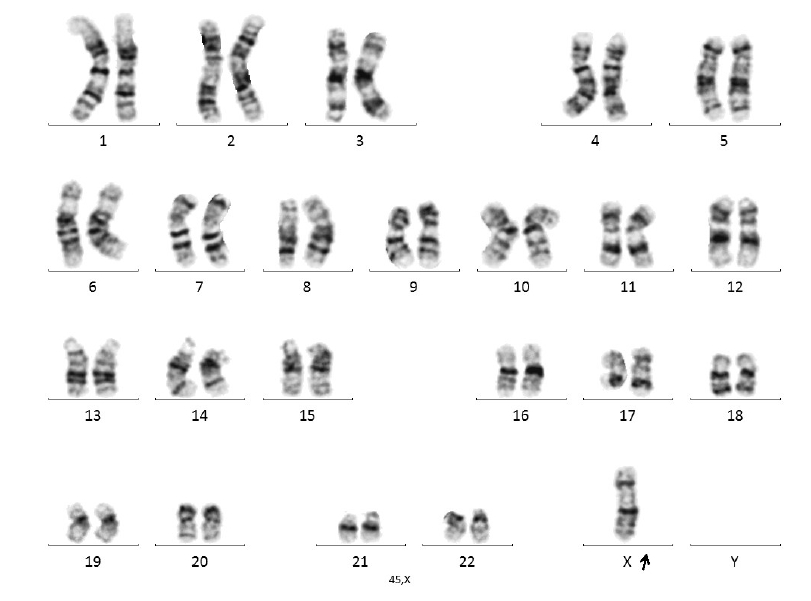
A 34-year-old right-handed woman presented with a sudden severe headache. She had a history of Turner syndrome for the last 20 years, which was managed with medical treatment, including estrogen hormone replacement therapy. Computed tomography revealed a SAH in the basal cistern (Fig. 1A). Routine cerebral angiography and 3-dimensional images demonstrated a saccular aneurysm of the right anterior communicating artery (Fig. 1B, C). The aneurysm was treated with endovascular coil embolization (Fig. 2). On admission, the patient underwent genetic analyses. One normal X chromosome was present in female cells, and the other sex chromosome was missing or structurally altered, compatible with Turner syndrome (Fig. 3). The patient recovered favorably without neurological deficits.
DISCUSSION
Turner syndrome is a chromosomal disorder that affects approximately 1 in 2,500 to 0 live births, is associated with a range of comorbidities involving the cardiovascular system, and affects both pediatric and adult patients. Vascular abnormalities, including aortic dilatation, dissection, and coarctation, are common in patients with Turner syndrome3,7,10,13,15,16). However, comorbidities involving the cerebrovascular system, such as cerebral aneurysms presenting with SAH are rare.
The exact cause and underlying mechanism of aneurysm formation and the growth and development of SAH in Turner syndrome are unknown. It was most likely the rupture of dilated vessels stemming from vasculopathy, characterized by an arterial wall defect, increased intimal thickening, and enlarged arteries1,7,8,11). Connective tissue defects, such as cystic medial necrosis of the arterial wall, are common findings in postmortem examination of Turner syndrome with spontaneous artery dissection. This finding is relatively common in cases of Turner syndrome complicated by histology 6,12). The arterial wall abnormalities in Turner syndrome are not restricted to the aorta. Arterial dilatation, enlargement, and increased intimal thickening, similar to those observed in the aorta, affect the cerebral arteries1,6,7). Theoretically, these underlying arterial wall abnormalities could lead to a higher risk of spontaneous aneurysm formation and rupture of the affected vessels in Turner syndrome1,3,4). Another explanation for cerebral aneurysms is that estrogen deficiency in patients with Turner syndrome may be hypothesized to contribute to intimal thickening, followed by outward remodeling and vessel enlargement. A growing body of evidence indicates a risk of aneurysm formation and SAH in women with estrogen loss, such as menopause5,7,11). Similar to all arteries, the cerebral arteries consist of three layers: the intima, media, and adventitia. The internal elastic lamina separates the intima from the media and is essentially a fenestrated elastin sheet. Collagen fibers are mainly produced by fibroblasts. Fibroblasts also produce, organize, and remove the extracellular matrix14). Collagen wasting, commonly observed in the bone and skin in the postmenopausal period due to decreased estrogen levels, could be responsible for the formation of aneurysms in the proximal segments of the cerebral arteries, as it occurs in various connective tissue diseases. Estrogen scavenges reactive oxygen species following endothelial injury and inhibits their formation11). Tightly regulated proteolytic degradation of the extracellular matrix is an important component of normal vascular homeostasis; however, if poorly controlled, it may contribute to the pathogenesis of cerebral aneurysms. Therefore, estrogen hormone replacement therapy may be an appropriate management strategy for early intervention in Turner syndrome to reduce the progression of intimal thickening and ultimately clinical atherosclerotic disease, although interventional studies are required to prove this point2,5,11,13). An other possible mechanism of cerebral aneurysms is the upregulation of transforming growth factor beta and matrix metalloproteinases, along with mutations in the gene loci for smooth muscle α-actin, which may also contribute to smooth muscle cell hyperproliferation in patients with Turner syndrome, resulting in vasculopathy of arterial wall defects, increased intimal thickening, and formation of aneurysm1,2,6,8,11). The incidence of hypertension and plasma renin activity is higher in Turner syndrome. The high plasma renin activity may be due to the renal vascular abnormalities of Turner syndrome. Therefore patients with Turner syndrome are susceptible to renovascular hypertension. Patients with Turner syndrome may develop vascular abnormalities in the renal and cerebral arteries due to chromosomal abnormalities. Both renovascular hypertension and cerebrovascular abnormalities may play a role in cerebrovascular incidents5,8,9).
CONCLUSION
Turner syndrome, associated with aneurysmal SAH, is a rare cerebrovascular anomaly. Our patient demonstrated the utility of genetic evaluation for patients with cerebrovascular disease and dysmorphism. Further investigations are needed to reveal the risk factors, vascular anatomy, and causative mechanisms of Turner syndrome with aneurysmal SAH.