INTRODUCTION
Marjolin's ulcers represent a unique subset of squamous cell carcinomas, emerging primarily within burn scars or chronic wounds and notorious for their aggressive malignant transformation2,4,6,11,13,18). Malignant tumors of the sacrum do not respond well to chemotherapy or radiotherapy. Therefore, wide surgical excision is considered the treatment of choice. Due to the invasiveness of the lesion, a multidisciplinary approach is required11). Although the lesion may occur at many different parts of the skin, carcinomas directly invading the sacrum are rarely reported4,11,13). Invasion to the sacrum complicates wide surgical excision due to the anatomical structure of complex blood vessels around the sacrum5). Therefore, a comprehensive understanding of the anatomy in 3-dimensional (3D) model is essential for effective surgical treatment.
The advent of 3D printing technology introduces a transformative solution to these challenges. By converting virtual 3D images into tangible models, 3D printing facilitates a deep understanding of both the general and pathological anatomy involved. This innovation has proven particularly valuable across various medical disciplines, including surgery, where it enhances surgical planning, efficiency, and outcomes. In neurosurgery, for instance, 3D-printed models have been shown to significantly improve surgical precision, reduce operation time, and decrease both intraoperative blood loss and radiation exposure. Such advantages are corroborated by numerous studies, highlighting the potential of 3D printing in revolutionizing surgical practice9,14,19).
This article presents a novel case of Marjolin's ulcer with direct invasion into the sacrum, successfully excised with the aid of a 3D-printed model. Through this case, we explore the application of 3D printing in addressing the surgical complexities posed by sacral involvement in Marjolin's ulcers, illustrating the practical benefits of this technology in enhancing operative planning and execution.
CASE REPORT
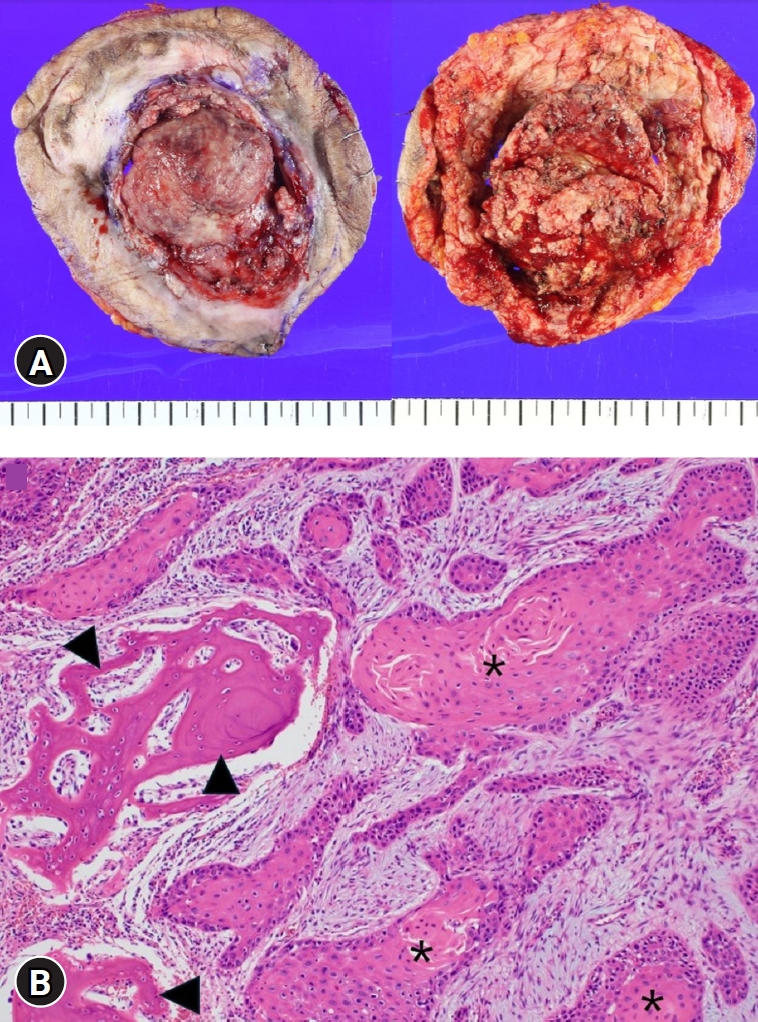
We report the case of a 48-year-old male with a history of quadriplegia following a diving accident in 1996, presenting with a progressively enlarging sacral mass. Initially observed as a quarter-sized sacral sore, conservative treatment was pursued without further diagnostic evaluation due to the absence of pain, bleeding, or discharge. Over six months, the lesion expanded significantly in size, prompting a punch biopsy that confirmed squamous cell carcinoma (Fig. 1).
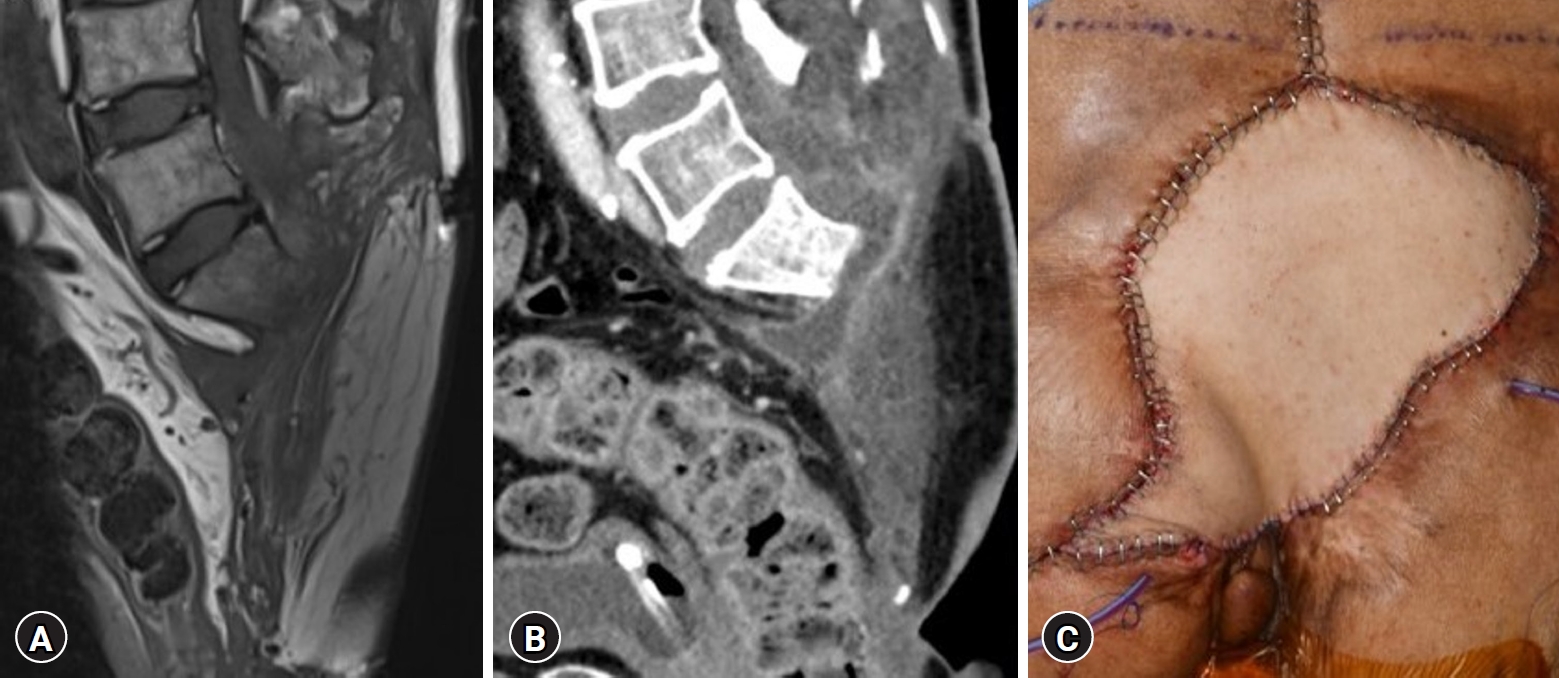
Magnetic resonance imaging (MRI) and computed tomography (CT) were conducted to assess the extent of the mass. The imaging studies revealed a lobulated mass measuring approximately 7 cm in size, accompanied by a significant soft tissue defect in the retro-sacral area at the sacrum S2-3 vertebral body level of the sacral spine. Notably, there was evident direct involvement of the S2-3 vertebral body and posterior elements, resulting in severe compression of the thecal sac (Fig. 2). These findings underscored the complexity of the tumor's anatomy and its challenging location. Given the intricate anatomy of this lesion, we utilized 3D-printed models to aid in surgical planning.
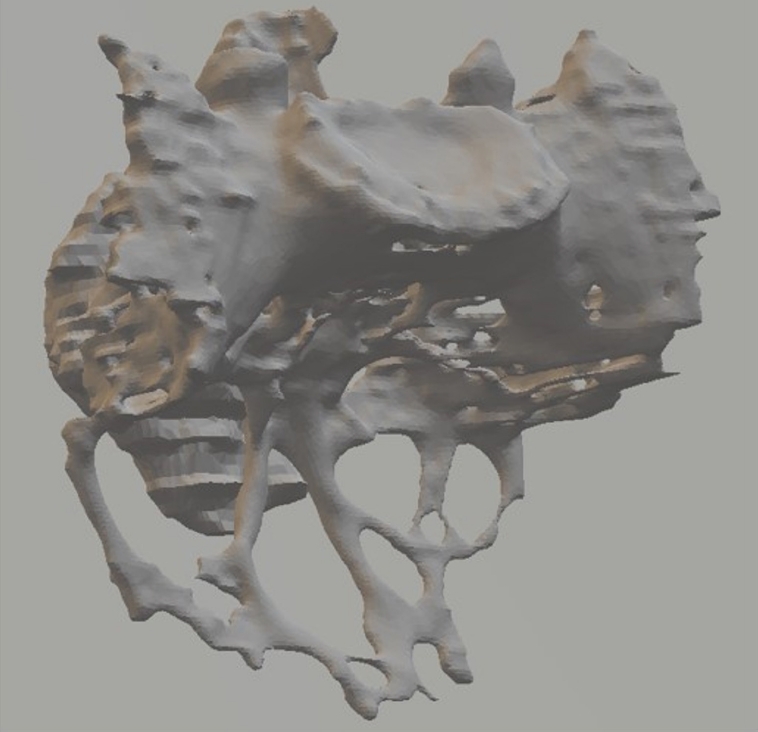
CT images were exported in standard digital imaging format and processed with Mimics medical image processing software (version 20.0; Materialise, Leuven, Belgium) to form the baseline 3D design. The 3D printing was performed with 156 mL of resin material (Fig. 3). Based on the imaging findings and the 3D-printed models, we planned the surgical procedure, which involved the removal of all tumors below the S1-2 disc level, as well as the normal anatomical structures surrounding the tumor. This approach aligns with that mentioned in previous papers on high partial sacrectomy, a surgical procedure that involves resection above the S3 level, based on the tumor location, without extending the resection up to the L5/S1 disc level7,15).
Prior to the surgery, a surgical plan was developed using a 3D-printed model to determine the extent of sacral resection. In the model, the main mass was highlighted in blue, while the surgical resection plan was indicated in pink (Fig. 4). The plan involved resecting approximately 1 cm from the margin of the normal bony structure, including the tumor, to ensure en bloc removal while minimizing the removal of the sacroiliac joint. Since the tumor did not invade the presacral structures, a posterior-only approach was chosen. The surgical procedure included S1 laminectomy and high partial sacrectomy below the S1-2 disc level while preserving both S1 nerve roots. Additionally, partial removal of the right side of the sacroiliac joint was performed. The frozen biopsy results confirmed that the surgical margin was free from tumor cells.
Following the high partial sacrectomy, the reconstructive plastic surgery team performed skin reconstruction using a microvascular free flap from the latissimus dorsi muscle. This approach was chosen due to the large size of the skin defect, which was not suitable for primary closure. Given the patient's ambulatory status, mechanical reconstruction was not pursued. Postoperatively, the patient experienced minimal changes in his neurological condition, with a slight improvement in defecation.
Histopathological examination of the surgical specimen confirmed the diagnosis of squamous cell carcinoma (Fig. 5). Postoperative CT and MRI scans, as well as the photo taken after surgery, confirmed the absence of tumor remnants and successful reconstruction with the latissimus dorsi musculocutaneous free flap (Fig. 6). An additional model was printed using postoperative imaging scans, which confirmed that the extent of resection matched the surgical plan outlined using the preoperative 3D-printed model (Fig. 7).
DISCUSSION
A Marjolin’s ulcer is a squamous cell carcinoma that can develop in any chronic wound. Wide surgical excision is the recommended curative treatment for Marjolin’s ulcers1). In our specific case, the Marjolin’s ulcer originated from a sacral pressure sore and invaded the sacrum. Therefore, we planned a wide excision that would involve sacrectomy. Sacrectomy is a challenging procedure, even for skilled neurosurgeons, due to the complex anatomy of the sacrum and its intricate relationship with surrounding structures such as bony structures, major blood vessels, and abdominal organs5,9,12,17). Additionally, it has been reported that sacrectomy can cause many complications, such as sacral instability, vessel injury, nerve injury, gastrointestinal tract injury, massive intraoperative blood loss and prolonged operative time17). These risks emphasize the need for meticulous surgical planning and execution.
In contemplating sacrectomy, the decision between anterior and posterior approaches hinges on tumor location and involvement of abdominal structures. The approach side is the first thing to decide. An anterior approach is recommended for tumors invading the abdominal cavity, intestines, and blood vessels, or sacrectomy of the mid-S2 or higher level is required16). Otherwise, the posterior approach is preferred. In our case, the tumor did not invade the presacral region nor the gastrointestinal tract. We decided to perform a posterior-only approach for sacrectomy.
There are some reports emphasizing that 3D printing is helpful for determining surgical plans19). Preoperative 3D printing aids in enhancing surgical planning and improves the accuracy of the actual surgical procedure14,19). The 3D printing is advantageous in that it allows a clear representation of the actual pathologic condition. By offering a tangible, precise representation of the pathological condition, 3D models surpass traditional 2D imaging in facilitating spatial understanding and surgical strategy formulation. This case reinforces the utility of 3D printing in enhancing surgical accuracy and decision-making, echoing findings from previous reports on its benefits in complex surgical interventions.
There are some case reports of surgically treated Marjolin’s ulcers or sacral tumors. Buchanan and Campbell3) reported the case of a patient who underwent coccygectomy for a challenging sacrum Marjolin’s ulcer and S4-5 sacrectomy due to recurrence of the Marjolin’s ulcer. Extended transpelvic vertical rectus abdominis myocutaneous flaps, bilateral gluteal flaps, and other muscles are used to fill the defect after the operation3). Similarly, Gaster et al.10) reported a case of recurrent pilonidal cysts and ulceration that was aggravated in a sacrum Marjolin’s ulcer. The patient underwent radical excision of squamous cell carcinoma and partial sacrectomy by oncologic surgeons, which resulted in a wound measuring 450 cm2 with an exposed rectum. Garcia-Tutor et al.8) reported that they used 3D printing in preoperative planning for the surgical flap of Marjolin’s ulcers and other oncologic conditions that require reconstruction surgery with either myocutaneous or fasciocutaneous flaps. They used Osirix software as a tool to evaluate the volume and dead space of the Latissimus dorsi flap.
The reported cases involving Marjolin’s ulcers and sacral tumors with and without 3D printing are summarized in Table 1. Until now, there have been no reports on the use of 3D-printed models in the preoperative planning of sacrectomy for Marjolin’s ulcer. Notably, our case contributes to the literature as the first documented use of a 3D-printed model in the preoperative planning of sacrectomy for a Marjolin's ulcer with sacral invasion. This innovation not only supported the successful tumor removal by a surgeon with limited sacrectomy experience but also underscored the potential of 3D printing to democratize complex surgical procedures, making them accessible to a broader range of practitioners.
The limited prevalence of Marjolin's ulcers and the absence of a standardized surgical protocol underscore the necessity for further research. The accumulation of cases utilizing preoperative 3D printing will be invaluable in refining surgical approaches for complex anatomical structures. Moreover, comparative studies on postoperative outcomes with and without the aid of 3D models could further elucidate the technology's impact on surgical success and complication rates.
CONCLUSION
A Marjolin’s ulcer is a rare disease that necessitates wide surgical excision and flap reconstruction. In cases where the sacrum is invaded, sacrectomy of the tumor and surrounding tissues is necessary. However, surgery poses challenges due to anatomical complexity, including that of various vessels and nerves. Nonetheless, utilizing a 3D-printed model, as in our case, can reduce the incidence of complications and assist even inexperienced surgeons in performing surgical removal with minimal complications.